Currently we are forming the editorial board
Leave a reply
Abstract
Background: The COVID-19 pandemic has disproportionately affected refugee populations, with refugees suffering higher rates of exposure and infection and a higher risk of severe disease and death due to socioeconomic disparities, reduced access to healthcare, and underlying medical conditions. Widespread vaccination is critical to reduce the individual morbidity and mortality as well as the public health burden of COVID-19. However, the uptake of COVID-19 vaccination among refugee populations is unknown.
Methods: We used validated surveys to quantitatively assess COVID-19-related fear and vaccine hesitancy in a population of Syrian refugees living in Turkey.
Results: COVID-19 vaccine hesitancy is critically high among Syrian refugees, with 85% of participants refusing vaccination. However, COVID-19 fear is also high, with over 90% of participants expressing fear of contracting or dying from COVID-19. Misinformation and false beliefs regarding vaccine efficacy and side effects contribute to the discrepancy between high fear of an infectious disease and low rates of acceptance of a life-saving preventive measure.
Conclusion: COVID-19 vaccine hesitancy is alarmingly high in Syrian refugee populations. Targeted interventions to improve vaccine acceptance in refugee populations are urgently needed.
Keywords
COVID-19, Vaccine hesitancy, Refugees, Syria, Turkey
Background
The COVID-19 pandemic has caused over 650 million recorded cases and over six million deaths worldwide as of December 2022 per World Health Organization statistics. Refugees and asylum-seekers have been disproportionately affected by all aspects of the pandemic. Refugees are at higher risk of initial exposure to SARS-CoV-2, are more likely to be hospitalized with COVID-19, and have a higher mortality rate compared to non-refugee populations [1]. A multitude of factors contribute to increased risk of in this population. Refugees are more likely to reside in crowded living conditions, to work low-wage public-facing jobs, to have less access to public health messaging in their native language, and to have lower health literacy compared to non-refugee individuals [2-8]. Once infected, refugees have a higher risk of severe COVID-19 symptoms, of requiring hospitalization due to COVID-19, and of death due to COVID-19. This is likely due to a higher incidence of chronic comorbidities, delays in seeking medical attention, and exclusion from the healthcare system, among other causes. Special attention to the effect of the COVID-19 pandemic on refugees is urgently needed.
Turkey harbors the world’s largest population of refugees and the world’s largest Syrian refugee population, with 3.65 million Syrian refugees and an additional 330,000 refugees from other countries [9]. Turkey has been profoundly affected by the COVID-19 pandemic, with over 12 million infections, nearly 92,000 deaths, massive inflation, and an unemployment rate of up to 40% [10]. Even prior to the pandemic, the refugee population in Turkey placed humanitarian and economic strain on the country. In 2020, the United Nations High Commissioner for Refugees (UNHCR)’s budget for refugees and asylum-seekers in Turkey was 365 million US dollars (USD); however, the sum of all available funds was only 131 million USD, a gap of 234 million USD [11].
Vaccination, combined with non-pharmaceutical methods such as social distancing and use of masks, offers the world’s best chance at curtailing the COVID-19 pandemic. Multiple effective and safe vaccinations to prevent COVID-19 have been developed and widely implemented with infection reduction rates of over 90% and excellent safety profiles. Unfortunately, vaccine hesitancy, defined by the World Health Organization (WHO) as “the reluctance or refusal to vaccinate despite the availability of vaccines,” is common in many populations. Given that refugees are at increased risk of COVID-19 exposure, infection, severe disease, and death, vaccination of this population is critically important, and vaccine hesitancy in this group is life-threatening. However, refugee and migrant populations have dismally low vaccination rates compared to non-refugee populations. Prior to the COVID-19 pandemic, vaccination rates for other preventable infectious diseases, such as measles-mumps-rubella (MMR), polio, and diphtheria-pertussis-tetanus (DPT), had been persistently low for decades in refugee populations compared to non-refugee populations [12]. With regard to the COVID-19 vaccine, as of June 2021, 85% of COVID-19 vaccine doses administered had been given in high- and middle-income countries, but 85% of refugees reside in developing countries [13]. Even within vaccine administration programs in developing countries, refugees are neglected: for example, in Lebanon in April 2021, refugees and migrants comprised 30% of the country’s population, but only 2.9% of vaccinated individuals [14].
Low COVID-19 vaccination rates among refugees are multifactorial. Some contributors are systemic, including lack of healthcare coverage or access to care for refugees, lack of vaccine information in refugees’ language, lack of transportation or financial means to obtain vaccination, and perceived fear of detention when presenting for medical care [15]. However, COVID-19 vaccine hesitancy is prevalent in refugee populations as identified by qualitative interviews [16]. These investigations identified misinformation and false beliefs as major drivers of vaccine hesitancy: for example, that COVID-19 is a hoax, that COVID-19 is a “Western disease,” that the government cannot be trusted, and that the COVID-19 vaccine contains microchips [17]. Facebook, TikTok, Whatsapp, and YouTube were cited as primary sources of COVID-19-related information [17].
Objectives
A rigorous understanding of the motivations, attitudes, and fears regarding vaccination is critically needed in order to decrease vaccine hesitancy and improve vaccination rates in refugee populations. In this study, we present the first quantitative investigation of refugee COVID-19 vaccine hesitancy using a validated questionnaire.
Methods
A cross-sectional survey was conducted in January 2022 among Syrian refugee patients in Turkey. Data were collected from patients aged 18 and older who presented for outpatient care at a public medical facility in Istanbul, Turkey. Patients who had already received any COVID-19 vaccine were excluded. Informed consent was obtained from each participant. This study was approved by the Institutional Review Board of XXX (IRB# XXX).
COVID-19-related fear was assessed via the Fear of COVID-19 Scale (FCV-19S). FCV-19S was developed in 2020 by a multinational group from Hong Kong, Iran, the United Kingdom, and Sweden [18]. FCV-19S assesses multiple aspects of fear related to COVID-19, including vulnerability to infection, fear of dying, and psychological and physical symptoms of anxiety. FCV-19S has robust psychometric properties and provides a reliable quantification of the severity of fear of COVID-19. Response patterns are not affected by respondent age or gender. The scale has since been implemented and validated in numerous other European, Middle Eastern, and Asian countries, including Turkey.
General vaccine hesitancy sentiment was assessed using the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunization (SAGE) definition. Assessment of vaccine hesitancy by the SAGE definition can be done via as few as three questions regarding vaccine behaviors; this definition and question set have been widely employed worldwide [19].
COVID-19 vaccine hesitancy was assessed using a version of the Vaccination Attitudes Examination (VAX) scale. VAX is a measure of anti-vaccination sentiment that was initially developed in 2017 by a cooperative group from the United States and New Zealand [20]. Initially developed to measure general anti-vaccination attitudes, the VAX scale can be adapted to assess attitudes toward specific vaccines. The original VAX scale has high internal consistency and validity, and responses are significantly associated with both past vaccine behavior and future vaccine intentions. The VAX scale has been adapted to create the Attitudes toward COVID-19 Vaccine Scale to assess COVID-19 vaccine hesitancy, and has been implemented in several countries, including the United States, France, and India.
For the present study, assessments were translated from English into Arabic, and participant responses were translated back into English. A pilot with 20 participants was initially performed. The questionnaire and the logistical arrangements were found feasible by the participants.
Statistical analysis: Statistical analyses were performed using SPSS statistical software version 24 (IBM Corporation, Armonk, New York, USA). Results are presented as frequencies and percentages for categorical variables and as the mean and standard deviation for continuous variables.
Results
A total of 321 participants were recruited to the study and completed the survey. The median participant age was 43 (range: 18-75). Forty-three percent of participants identified as female. The majority of participants were illiterate (60%), were not working (62%), and lived in large households (household size of five to six, 41%; household size of seven to nine, 42%). Thirty percent of participants reported a personal history of COVID-19 infection. Twenty-seven percent of participants reported a personal history of diabetes mellitus, hypertension, and/or hyperlipidemia. Demographic characteristics of the cohort are displayed in Table 1.
Table 1: Demographic characteristics of study participants
|
Median (range) |
|
| Age | 43 (18-75) |
| N (%) | |
| Gender identity | |
| Female | 139 (43.3) |
| Male | 182 (56.7) |
| Education | |
| Illiterate | 193 (60.1) |
| Primary school graduate | 71 (22.1) |
| Secondary school graduate | 57 (17.8) |
| Work status | |
| Not working | 200 (62.3) |
| Working irregularly | 41 (12.8) |
| Working regularly | 80 (24.9) |
| Size of household | |
| 3-4 | 57 (17.8) |
| 5-6 | 130 (40.5) |
| 7-9 | 134 (41.7) |
| Personal history of COVID-19 infection | |
| Yes | 94 (29.3) |
| No | 227 (70.7) |
| Personal history of chronic disease (DM, HTN, and/or HLD) | |
| Yes | 86 (26.8) |
| No | 235 (73.2) |
Fear of COVID-19 was common among participants, as assessed by FCV-19S. Ninety-three percent of participants reported feeling uncomfortable when thinking about COVID-19, and 75% of participants reported fear of dying of COVID-19. Forty to 65% of participants also reported physical symptoms of anxiety (palpitations or insomnia) related to fear of COVID-19. Results of the FCV-19S assessment are displayed in Table 2.
Table 2: Fear of COVID-19
|
Yes [N (%)] |
No [N (%)] |
|
| I am most afraid of Coronavirus-19. | 300 (93.5) | 21 (6.5) |
| It makes me uncomfortable to think about Coronavirus-19. | 300 (93.5) | 21 (6.5) |
| My hands become clammy when I think about Coronavirus-19. | 180 (56.1) | 141 (43.9) |
| I am afraid of losing my life because of Coronavirus-19. | 239 (74.5) | 82 (25.5) |
| When watching news and stories about Coronavirus-19 on social media, I become nervous or anxious. | 218 (67.9) | 103 (32.1) |
| I cannot sleep because I’m worrying about getting Coronavirus-19. | 127 (39.6) | 194 (60.4) |
| My heart races or palpitates when I think about getting Coronavirus-19. | 207 (64.5) | 114 (35.5) |
General vaccine hesitancy was common among participants. Seventy-one percent of participants reported refusing a vaccine for themselves or their child in the past, and 46% reported postponing a vaccine recommended by a physician. Vaccine hesitancy data are displayed in Table 3.
Table 3: Vaccine hesitancy
|
Yes [N (%)] |
No [N (%)] |
|
| Have you ever refused a vaccine for yourself or a child because you considered it as useless or dangerous? | 229 (71.3) | 92 (28.7) |
| Have you ever postponed a vaccine recommended by a physician? | 147 (45.8) | 174 (54.2) |
| Have you ever had a vaccine for a child or yourself despite doubts about its efficacy? | 0 (0) | 321 (100.0) |
COVID-19 vaccine hesitancy was high among participants. Only 14% of participants stated that they would receive the COVID-19 vaccine. The remaining 86% of participants stated that they would refuse the COVID-19 vaccine. Of those respondents who refused vaccination, reasons for refusal were fear of side effects (78.5%), doubt about effectiveness (19%), and suspicion of short production timeline (2.5%). Attitudes toward COVID-19 Vaccine Scale response data are displayed in Table 4.
Table 4: Intentions regarding COVID-19 vaccination
| If a vaccine against the Coronavirus was available, would you get vaccinated? |
N (%) |
| Yes | 46 (14.3) |
| No | 275 (85.7) |
| If no, why? | |
| Fear of side effects | 216 (78.5) |
| Doubt about effectiveness | 52 (19.0) |
| Suspicion of short production timeline | 7 (2.5) |
Discussion
In this study, we present the first quantitative assessment of COVID-19 vaccine hesitancy and fear of COVID-19 in a refugee population using validated questionnaires. COVID-19 vaccine hesitancy is alarmingly high in this population: 86% of participants stated that they would refuse a COVID-19 vaccine. General vaccine hesitancy is also prevalent in this population, with more than 40% of participants reporting a history of refusing or postponing a recommended vaccine.
The prevalence of vaccine hesitancy in this large cohort of refugee patients is concerning given this population is at extremely high risk in every phase of an infectious pandemic, from initial infection to death. Firstly, migrants and refugees are at higher risk of infection with the Coronavirus compared to non-refugee populations. For example, in Denmark in May 2020, the incidence of COVID-19 in the migrant population was 240 per 100,000, compared to 128 per 100,000 among native Danish individuals [21]. Similarly, in Spain in April 2020, the incidence of COVID-19 in the migrant population was 8.81 per 1,000, compared to only 6.51 per 1,000 for native Spanish individuals [22]. The living conditions of refugees, which commonly involve camp-type settings with crowding and extensive use of shared spaces, likely contribute to the increased incidence in refugee populations: outbreaks have been observed in migrant shelters in many countries. Even in non-camp settings, refugees are more likely to reside in shared or overcrowded housing. For example, in a survey of Organization for Economic Cooperation and Development (OECD) countries, migrants were twice as likely to live in an overcrowded housing setting (17%, versus 8% of native-born individuals) [1]. Occupational risks also contribute to increased risk of contracting COVID-19 among refugee populations: refugees are more likely to be employed in public-facing jobs, such as retail, delivery, hospitality, and transport, thereby increasing the risk of COVID-19 exposure compared to other, non-public-facing jobs [23]. Furthermore, refugees generally have more tenuous financial means compared to non-refugee populations and are more likely to be employed in “no work, no pay” jobs such as those mentioned above, necessitating the continuation of work even in high-risk conditions [4,5,23].
Refugees are also at higher risk of hospitalization and mortality from COVID-19. In Denmark in September 2020, migrants made up 15% of COVID-19-related inpatient admissions, despite comprising only 9% of the population [21]. In Sweden, the relative risk of ICU admission for COVID-19 was five times higher for migrants from Africa and the Middle East than for native Swedish individuals [24]. Similarly, in Norway, the incidence of hospitalization due to COVID-19 was 147 per 100,000 in migrant populations, compared to 37 per 100,000 for native Norwegian individuals [2,25]. Certain ethnic groups are at even higher risk of poor outcomes, and studies specific to Syrian refugees have found dismal COVID-related mortality rates. In Sweden, Syrian migrants had a relative risk of death from COVID-19 of 6.14 compared to native Swedish individuals [26]. Excess mortality in Syrian migrants in Sweden was 220% in 2020, due overwhelmingly to COVID-19 deaths [26].
Thus, given the high risk of initial exposure, severe disease, and death in this population, the magnitude of benefit from vaccination in this population is enormous, and the consequences of vaccine hesitancy are catastrophic. For example, the resurgence of measles in the United States, Norway, and other countries in the early 2000s as a result of increased parental refusal of MMR vaccination was notable for outbreaks heavily concentrated in migrant and refugee populations. In two outbreaks in Minnesota, USA in the 2010s, 72% of cases occurred in members of the Somali community [27,28]. During this time period, MMR vaccination rates among two-year-old Somalis in Minnesota fell to 54%, from over 90% ten years prior [29]. Similarly, in a 2011 measles outbreak in Oslo, Norway, 80% of cases occurred in members of the Somali community, in which MMR vaccine rates were also noted to be low [29,30]. Unfortunately, the present study confirms that vaccine hesitancy continues to be a major barrier to vaccination among refugee communities with regard to COVID-19 vaccination. Interventions to increase vaccine uptake in refugee populations are critically needed.
Vaccine uptake can be improved by addressing each contributing factor to low vaccination rates. Systemic factors must be addressed on the institutional level. For example, although the national COVID-19 vaccine program in Turkey, the setting of the present study, includes all individuals living in the country regardless of immigration, refugee, or asylum-seeking status, public health and vaccine programs in some countries exclude refugees, either explicitly, or indirectly due to requirements for identification or documentation to be presented at the time of vaccination. Removing systemic barriers by making COVID-19 vaccines available to all individuals regardless of legal status, improving outreach in refugees’ native language, increasing vaccine convenience, and guaranteeing protection from detention when seeking healthcare will all increase vaccination rates in individuals who desire to be vaccinated.
However, the present study identified that unvaccinated individuals who desire to be vaccinated (but may be impeded from doing so by systemic factors such as those detailed above) are a small minority among the Syrian refugee population in Turkey; the vast majority of participants are refusing COVID-19 vaccination, with concern for side effects the most commonly cited reason for refusal. Therefore, removing systemic barriers to vaccination is not sufficient to improve vaccination rates. Education on vaccine effects must be provided and misinformation and false beliefs must be addressed to improve vaccine hesitancy.
Although the present study is the first to quantitatively assess COVID-19 vaccine hesitancy in refugee populations using validated questionnaires, vaccine hesitancy in general has been well-studied. The most effective strategies for reducing vaccine hesitancy and improving vaccination rates overwhelmingly involve accessible, understandable health education from trusted sources. These strategies have been well-described by previous groups [31,32]; we briefly summarize the most common and salient points here. First, and perhaps most importantly, public health messaging must be available in refugees’ native language. In Turkey, a robust COVID-19 public health program is available via internet and a COVID-19 hotline is available via telephone, but these sources are only available in Turkish and English; 80% of Syrian refugees speak only rudimentary Turkish. An Arabic translation of the website or an Arabic language option for the telephone hotline would make this information more accessible for Syrian refugees. This model has been extremely successful in Sweden, where healthcare workers use telemedicine platforms nicknamed “Corona lines” to distribute COVID-19 educational information, triage respiratory symptoms, and instruct patients on appropriate quarantine and hygiene in Arabic, Somali, Tigrinya/Amharic, and Persian/Dari as well as the Swedish national languages. Second, vaccine development, testing, and approval information should be transparent and accessible to the public. As prior qualitative interviews cited above noted social media as the main source of COVID-19-related information for refugees, this information should be publicized via not only traditional media, but verified sources on social media as well. For example, national health ministries can use their official Facebook and other social media feeds to publicize vaccine information; this information should be in refugees’ native language, as discussed below. Specific provocative or culturally relevant false beliefs, such as concern that the vaccine contains pork products or causes infertility, should be targeted and addressed emphatically. The participants in the present study overwhelmingly indicated fear of side effects as the reason for vaccine refusal; public health information should emphasize the favorable side effect profile of COVID-19 vaccines. Third, personal storytelling from persons with whom refugee populations identify are effective means of appealing to individuals’ empathy and emotion. For example, for a target population of Syrian refugees, a public health announcement featuring a multigenerational Syrian family who accepted the vaccine can be filmed and widely publicized as described above. Fourth, community leaders, particularly religious leaders, such as imams at Syrian-majority Arabic-speaking mosques, should be partnered with for the dissemination of vaccine information. Fifth, refugee populations should be actively included in the process of public health education and information dissemination; for example, local public health committees should include at least one refugee member who participates in vaccination campaigns.
We found that fear of COVID-19 is also common in this population, with over 90% of participants reporting COVID-19-related fear. Notably, 75% of participants stated that they fear dying of COVID-19. The coexistence of high COVID-19 fear with high vaccine hesitancy seems contradictory. This contradiction emphasizes the role of misinformation, portraying the preventive measure as more harmful than the disease itself, in promoting vaccine hesitancy in this population. However, COVID-19 fear may become a motivation for participants to agree to vaccination if misinformation is replaced with accurate information about the efficacy and safety of COVID-19 vaccines.
The limitations of our study include its design as a cross-sectional survey, which represents the attitudes of the survey participants at one time point, and does not assess changes in attitudes over time. The demographic and clinical variables assessed, such as comorbidities and history of COVID-19 infection, were self-reported by participants, and were not verified by the investigators. The study was restricted to Syrian refugees in an urban metropolis. It may not be generalizable to other ethnic refugee populations, or to refugees in rural areas.
Conclusion
Refugee populations are at high risk of COVID-19 exposure, infection, severe morbidity, and mortality. Fear of COVID-19 infection is high in this population, with over 90% of participants reporting COVID-19-related fear. However, despite high levels of fear the disease, COVID-19 vaccine hesitancy is contradictorily and critically high among Syrian refugees in Turkey, with over 80% of individuals refusing vaccination. Fear of side effects is the most common reason for refusal of vaccination. Targeted public health outreach interventions are critical to improve vaccination rates in this vulnerable population.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Verbal and nonverbal communication generates various debates and feelings between individuals, finally improving knowledge and experiences and, last but not least, influencing people’s health. Mental activity is mainly influenced by visual, sound, and smells perception. A person’s appearance, colour use, scent, and movement in a specific environment create diverse motion pictures going along with excitement, indifference, or discomfort, according to data processing. The music expresses various themes; miscellaneous musical compositions decoded by matching corresponding musical instruments or human voices determine emotions, relaxation, and even attentiveness. Verbal communication skills are necessary to improve an individual’s professional, cultural and social life; the words’ meaning and energy influence people’s well-being. The effects of the usage of the words in the written format are different from the spoken words since the speech energy, controlled by the nervous system, adds value to the words’ significance. Communication skills by terms make a difference between individuals and initiate numerous actions according to their relevance, physical characteristics of words’ transmission, intended recipient’s sensitivity, and context.
In this digital era, an individual can put an idea in a writing format or convert it into a say that instantly goes up to the intended recipients using IT devices.
Speech or the words’ ordering analysis offers information about the individual:
Speech depicts its coordination in appearance; deficiencies at various levels for command and execution pathways indicate the voice’s signs of interest in clinical practice. Voice characteristics combined with the breathing data reflect blood flowing in the human body. Heart activity, the respiratory system’s function, and gravitational waves influence human body fluids movement; the digestive, endocrine, skeletal, respiratory system, kidney, and liver functions influence blood composition. The mind activity affects all these variables interplay, conveying the words and voice expression. Even so, the heart function and respiratory system, both under nervous system coordination, are seen as significant contributors to the voice function. Heart failure modifies the body’s fluid distribution and, subsequently, voice characteristics that change from one stage to another in its evolution.
Each person’s voice is distinctive and adaptable to various internal and external stimuli. AI supply leads to fast voice analysis and prediction of disorders in appearance or evolution. In this digital era, a video visit or only a phone call visit can offer sufficient details about individuals, including data health. For the medical team, an e-visit may be considered appropriate when necessary. For the patient, an in-person or e-visit represents a convenient option to get care in need. The patient experience can be appreciated /measured by his words’ composition to express gratitude, voice attributes, and sentiment analysis, preferably using AI supply. Subjective voice analysis and artificial intelligence utilization offer another perspective in clinical practice. Recent medical literature highlights ambitious AI projects for using the voice function in diagnosis. Therefore, according to individual financial status, there will be a wide range of options for the disease’s management in clinical practice. But only by using a mobile phone can the patient and the physician be connected to successfully control the patient’s disorders. The art of using the voice for analysis and decisions in clinical practice defines us as professionals in the community we serve.
Abstract
Purpose: The purpose of this Quality Improvement (QI) project was to complete a formative evaluation of Trauma Informed Care (TIC) content delivered in a population-focused health nursing course for senior-level undergraduate nursing students.
Methods: This was a descriptive study that gathered feedback from students about the Trauma Informed Care content. A survey was disseminated via Qualtrics after the module/lecture to gather information about the effectiveness of the lecture with respect to TIC content; timing of the lecture in the semester relative to clinical; attitudes/perceptions about the importance of the content and practical application.
Results: The content provided to the students in Nursing 466 Community Health improved students’ knowledge and skills related to providing Trauma Informed Care. Twenty-five participants from the Bachelor of Science in Nursing program at Gonzaga University participated
Keywords
Bachelor of nursing students, Trauma-informed care, COVID-19, Population health
Introduction
Current times require us to reexamine the content we are teaching community/public health nursing courses. The American Association of Public Health suggests that undergraduate public health nursing education should include information on trauma-informed care. Trauma-informed pedagogy in public health is not new, but the trauma related to the COVID-19 pandemic argues for making it a priority for all educators [1]. As a result of the pandemic many in the public have experienced trauma related to stress, financial impact, mental health, and physical well-being. We are faced with increasing rates of the COVID-19 pandemic, chronic conditions, infections, violence, and extreme weather events. All these circumstances point to a growing need for including content about Trauma Informed Care. The concept of trauma can be described as the following “Individual trauma results from an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life-threatening and that has lasting adverse effects on the individual functioning and mental, physical, social, emotional, or spiritual well-being [1]. This article reports the formative evaluation of adding content about Trauma Informed Care (TIC) to a population-focused health course in a Bachelor of Science (BSN) program at a private university in the inland northwest. Trauma-informed care is grounded in a set of four assumptions and six key principles as a framework. The four Rs of this Trauma-Informed Approach framework are: realize, recognize, respond, and resist re-traumatization [1]. “A program, organization, or system that is trauma-informed realizes the widespread impact of trauma and understands potential paths for recovery; recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and responds by fully integrating knowledge about trauma into policies, procedures, and practices, and seeks to actively resist re-traumatization (wording bolded in original text). These concepts are needed when working in population health. The content that was presented to this BSN group of students was organized into three sections. Section 1 was an overview of trauma-informed care, including the definitions of trauma and passive trauma. The trauma that those who experience homelessness or living in poverty were used as exemplars. This section included an overview of neurobiology, biopsychosocial needs of those experiencing homelessness, addiction, and/or poverty, and how the brain reacts to trauma. Section two described different types of traumas as a public health issue of our time and included an overview of Adverse Childhood Effects (ACEs). Exemplars of trauma related to ACES, as well as the pandemic, and natural disasters were presented. Section two also included an overview of current statistics related to trauma and how stress affects those that experience trauma. Section three addressed addiction, stress, and homelessness, how to return to a state of hope, how to implement and “do” trauma-informed care, transformation, and post-traumatic growth, and how not to re-traumatize individuals. Today we are not only faced with increasing diseases but also other traumatic events [2]. These events can be additional sources of trauma and Post Traumatic Stress Disorder (PTSD) in public health. Although the need for nurses who can manage care along a continuum, implement evidence-based practice, work in multi-disciplinary teams, and integrate clinical expertise with knowledge of community resources is recognized, there is a lack of pedagogy that includes Trauma Informed Care [3]. This article describes the need for gathering formative information to add trauma-informed pedagogy to the current community health course. Using that formative information students provide could lead to changes made to the content before presenting it to the next group of students. The TIC content and knowledge could be implemented with the partnership between the school of nursing (SON) and local agencies where students complete public health clinicals.
Background
As a result of the COVID-19 pandemic, there is an essential need to prepare BSN students to not only care for individuals, but also for populations. According to SAMSHA “PHN practice is population-focused and requires unique competencies, skills, and knowledge. The important skills of analytic assessment, program planning, cultural competence, communication, leadership, and systems thinking, and policy are critical to the PHN role” [4]. Considering the pandemic, students’ interest may be piqued, and more students now see public health as a viable career option. It is important as faculty to recognize how Public Health will be taught in the aftermath of the COVID-19 pandemic and have awareness of the trauma students could experience as new nurses taking care of COVID patients. The pandemic will have likely affected students as well as those prone to experience trauma among the population on a personal level either because they have become ill themselves or know someone that was affected by the virus. Furthermore, we need to consider the trauma of providing nursing care as a student to COVID patients. With this comes the need for trauma-informed care. Those from marginalized communities, the homeless population, and middle-class families have all been prone to traumatic experiences. Trauma Informed Care will ensure that the students gain knowledge and learning tools to serve their community with the knowledge of what Trauma Informed care is and how to reduce the risk of re-traumatization of clients [3]. The added pedagogy included Trauma Informed Care, to an already packed course that includes Disaster Preparedness, prioritizing social determinants of health, and the use of politics and policy. As faculty teaching, this group of “post-pandemic” students requires our pedagogy to include trauma-informed care so as to not exacerbate the client’s trauma in their public health clinicals’. The students at this school of nursing work in partnership with community sites such as shelters, homeless centers, the department of health, and many other agencies that provide services to populations that experience extreme poverty. The content took on a hybrid format of teaching online and in the classroom. Study findings provide information to inform revisions to the lecture to better meet the needs of students regarding this content.
Problem
Undergraduate Nursing students in this BSN program need Trauma Informed Care content. There is a gap in practice in the literature regarding Trauma Informed Care (TIC) taught in the BSN program. As a result of the COVID-19 Pandemic, many in the public may have experienced some form of trauma. There is a recurring recommendation from the American Public Health Association to start integrating TIC into the undergraduate curricula to educate BSN students on what Trauma Informed Care is and how to apply it to practice. This Quality Improvement Project aimed to examine the formative feedback and perceived value of the TIC content integrated into the BSN Community Health content.
Methods
This was a descriptive study within one BSN program. Students were enrolled in the senior-level community health class. Participation was voluntary and consent, as well as understanding the purpose and process of this project, was presumed by completion of the survey. Approval from the university’s IRB was obtained. The survey included both scaled and open-ended questions and students could voluntarily participate post-lecture. This article describes the preliminary findings of the perceived value of the TIC content and how students responded to the content delivered. The overall goal was to gather feedback about the effectiveness of the lecture and what changes need to be made for the future integration of TIC into the community health course. Participants were invited to participate in a Qualtrics survey sent out securely to their student email addresses during class by a staff member from the Dean’s Office. The investigator did not utilize email addresses herself but had the staff member send the surveys via email during class time from a remote location. The class roster was available to the staff member in the university system. Email addresses were not stored in any other system except for Qualtrics, the survey software. Once the survey and project were completed using Qualtrics, any email addresses used by the system were deleted. The investigator/course instructor informed the class (potential subjects) about the survey and study goals immediately before the lecture was given and informed the students of their ability to opt-in/out of the survey portion of the class, which occurred after the lecture was given. The survey consisted of 9 questions Likert-type scaled responses and 5 open-ended questions that were designed to gather feedback about the effectiveness of the lecture with respect to content; timing of the lecture in the semester relative to clinicals’; perceived importance of the content and practical application; information necessary to inform revisions to the lecture to make it tailored to the population-level needs of the students A Likert scale was used to gather quantitative data. Five of the questions were open-ended so that the students could provide written feedback exploring contextual factors [5,6]. Students’ narrative responses provided essential information about how to format the content and presentation for the next group.
Results
The Trauma Informed Care content is particularly valuable. This information also provides resources and tools for clinical practice use. The formative evaluation process used in the project provided valuable feedback to increase the quality of this content and delivery in the future to the next group of participants (students). The content provided to the students in Nursing 466 Community Health improved students’ knowledge and skills related to providing Trauma Informed Care. Twenty-five participants from the Bachelor of Science in Nursing program at Gonzaga University participated. Participating evaluators indicated that the education program was effective with respect to TIC content, the timing of the lecture in the semester relative to clinical, attitudes/perceptions about the importance of the content and practical application. Overall, 52% of participants felt the content was very understandable and 64% felt the content was very important to clinical practice. 56% of participants felt that the lecture was very understandable and 64% of the participants felt that the content was important to clinical practice. Participants (54%) felt that the content was usable in their practice and 44% of participants felt that it would impact their values and beliefs.
Demographics
Thirty-six students were enrolled in the course; 25 (69%) of participants completed the survey. This section outlines descriptive statistics performed for the Likert-type items that were a part of the questionnaire. To capture the students’ perceptions about the lecture, we included in the questionnaire questions such as “How informative was the lecture content” and “How relevant is this lecture to public health.” These questions were measured utilizing a Likert-type scale ranging. 0=Unimportant, 1=Somewhat important, 2=Moderately important, 3=Important, 4=Very important, 5=I don’t know.
Qualitative feedback identified strengths in the use of the open-ended questions related to how the lecture impacted the students’ values and beliefs about people who live with homelessness and substances; the length of the presentation; timeliness of the presentation; understandability of the lecture and lastly, what changes the participants suggested to improve the lecture for future students
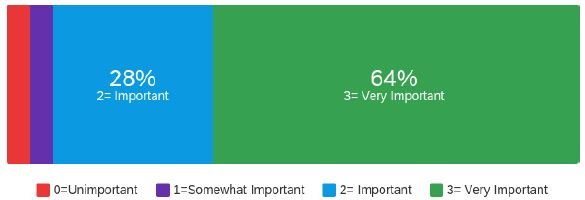
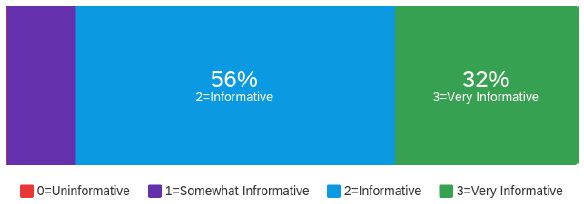
14 (56%) of respondents indicated that they found the lecture content to be informative, while 8 (32%) found it very informative. 21 (84%) of respondents found the lecture to be very relevant to the landscape of public health (Graph 1).
Graph 1: How informative was the lecture content
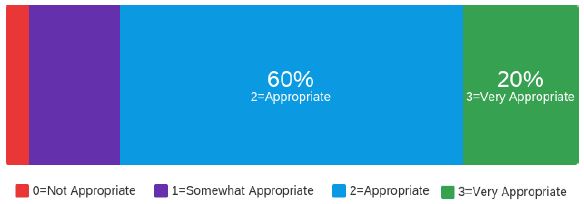
The students were asked to assess the length of the presentation. There were 25(60%) respondents that found the length of the presentation appropriate, while 5(20%) found it very appropriate (Graph 2).
Graph 2: Length of lecture
From this question, four different themes came to light. These themes are “different parts of the lecture “extending the lecture” “reduction in the lecture” and “additions to lecture.
The lecture was split up into three different sections and the students responded favorably to this and stated that “the presentation blended well together, and each section built off one another in a coherent manner”. There were some comments to extend the lecture by including more breaks and breaking apart what trauma-informed care is based on evidence-based practice and how that can be implemented in different communities. Related to the reduction in lecture the lecture was very consolidated, and students felt that there were a few slides that could be omitted. Some students suggested that perhaps it could be a multiday lecture. Additions to the lecture included suggestions to add some more videos and to include the ACE’s resources and some CDC resources.
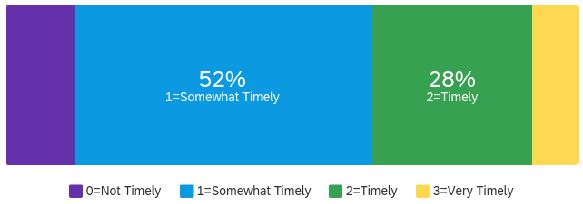
The timeliness of the lecture relative to the student’s clinical experiences was also assessed. There were 13 (52%) respondents that indicated that the lecture was somewhat timely;7 (28%) of respondents rated it as timely with respect to how early it was offered in the course (Graph 3).
Graph 3: Timeliness of the lecture
Timeliness was very important to the students, and they noted that it would be good for students to benefit from the content much earlier in their BSN curriculum. Students suggested receiving this content earlier in the semester of their program. It was stated that if they had this before their senior practicum it would be very beneficial. Others stated that they could see this content being threaded throughout their 4-year program. It was mentioned that trauma-informed care is something they are thankful they learned in their BSN track and wished to learn about it earlier.
To assess the impact of the lecture, the following questions were asked: “How understandable was the presentation?” 14 (56%) Respondents felt the presentation was very understandable (Graph 4).
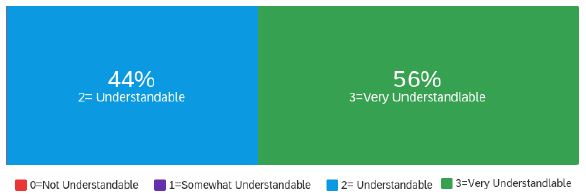
Graph 4: How understandable was the lecture
In response to this question Students mentioned that the topic was very relevant and helped them to see the “bigger picture”. Furthermore, they stated it would help them to identify paying attention to the information relating to ACEs among children, and being able to be an advocate for their patients was very important and helpful. Regarding the enjoyability of the lecture, students felt the PowerPoint was easy to follow and enjoyable to view.
“How important will this lecture be to your clinical practice,” 7 (28%) respondents felt that this was very important content for their clinical practice. 16 (64%) of respondents felt that this was very important content for their clinical practice (Graph 5).
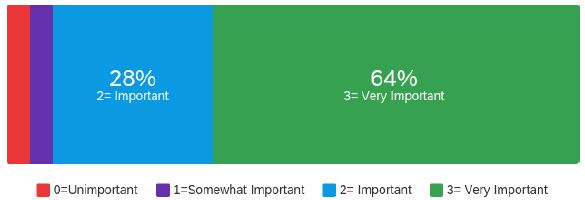
Graph 5: Importance of lecture to clinical practice
“To what extent do you feel the content can be used by you in practice immediately?” 9 (36%) of respondents felt that the content could be used in practice immediately. 13 (52%) respondents felt that the content was usable for practice immediately (Graph 6).
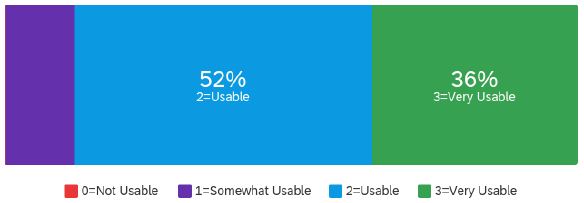
Graph 6: Usability of lecture in practice
“To what extent did the lecture content impact your values and beliefs about people who live with homelessness and use substances?” 9(35%) of respondents felt that the content was very impactful and related to the above question. 11 (44%) of respondents felt it was impactful content (Graph 7).
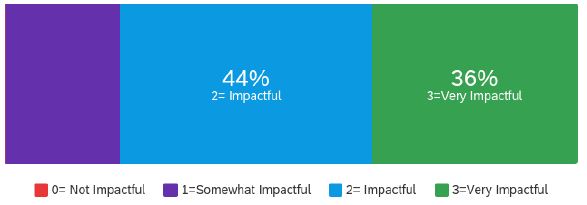
Graph 7: Impact on values and beliefs
The first question analyzed reflects the impact that the content on the student’s values and beliefs about how people live with homelessness and substances. Students stated that the content was “extremely relevant” and is a significant component in promoting healing. Furthermore, students stated that “being educated on this topic allows us to be more aware and educate the community we work with during our community health clinical’ as future nurses, and it provides details about the struggles the homeless face since many of those experience some form of trauma that have been homeless before.” There were two sub-questions to this overall question.
What changes would you make to the TIC lecture to improve it for future NURS 466 students? This question addressed any suggestions or changes to the lecture. Three themes emerged including resources, timing, and methods. Students suggested that they could offer specific resources or reference for patients or clients. They also asked how they can be sure to not re-traumatize patients. One of the students suggested asking someone who experienced trauma and overcame it to write a letter and share how they overcame their trauma. Timing again addressed the fact students wanted this content earlier in the semester, and program. Regarding methods, students mentioned more class discussions and asked for some real-life clinical examples. They also suggested part of the lecture be more interactive and include discussion.
Outcomes
Participating evaluators indicated that the education program was effective with respect to TIC content, the timing of the lecture in the semester relative to clinical, attitudes/perceptions about the importance of the content and practical application. Receiving formative evaluation to improve the development of a trauma-informed public health education program that provided evidence-based strategies and resources was the primary goal of this project. The results of the program demonstrated the effectiveness of using formative evaluation to develop a trauma-informed educational lecture for senior undergraduate Bachelor of Nursing students. The educational lecture overall demonstrated positive responses as to how the lecture impacted the students’ values and beliefs about people who live with homelessness and substances; the length of the presentation; timeliness of the presentation; understandability of the lecture and lastly, what changes the participants suggested to improve the lecture for future students. The findings of this educational lecture resonate with findings from other publications in relation to the importance of educational content on trauma-informed care for undergraduate nursing students to equip students with knowledge and understanding of trauma-informed care as it relates to public health. Emphasis on how timely this lecture was given is noted and will help change the timeliness of future lectures provided at the beginning of the student’s semester rather than toward the end.
Limitations
While the development of this Trauma-Informed care lecture reasonably provides strong evidence of the effectiveness of using formative evaluation to aid the development of the lecture within the sample population, it has some limitations. The first limitation is that it did not provide pre- and post-feedback as to what knowledge base the students had related to the content. It was limited only to one class in the undergraduate nursing program and the feedback is provided at the end of class when students are overloaded with the information they just received.
Future Directions
To overcome some of the limitations the respondents in the next part of this project will have a pre-and post-survey. The formative information provided in this project will better the lecture offered to the next student group in the Spring 2021 semester.
Funding
There was no funding involved for this project.
Conclusions
The trauma-informed care for public health lecture developed for senior undergraduate nursing students is powerfully applied by using evidence-based content and resources poised to provide an excellent delivery system for educating students. The lecture provided students with evidence-based content related to how trauma-informed care impacts public health. The student participants’ responses to the formative evaluations in developing this content were positive. In addition, the responses provided positive feedback and suggestions to improve the development of this lecture for future students.
References
Abstract
We investigated the spike protein-specific IgG antibody levels against COVID-19 in a 64-year-old male medical staff periodically after two doses of COVID-19 vaccination and a third booster shot during a one-year period. The antibody levels increased after the two doses vaccination; however, it rapidly decreased in the first 3 months. The antibody levels increased again after the third booster vaccination. The antibody levels were remarkably higher than that after the two doses of vaccination and remained high for several months. We demonstrated that the third booster shot was significant in maintaining a high level of immunity against COVID-19.
Keywords
COVID-19, Vaccine, Antibody, Spike protein, Booster
Introduction
The COVID-19 pandemic [1], which began in early 2020, affected the examination and treatment of patients in hospitals, healthcare, and nursing care facilities in various ways. Vaccination for COVID-19 [2-4] initially started in the United Kingdom in December 2020 and subsequently started in Japan in February 2021, which has been effective in preventing the onset and reducing the severity of the disease [5-7] owing to its high immune induction potency [8]. However, some cases of breakthrough infections have been reported [9-11], and it has been pointed out that one of the causes is a decrease in the levels of antibodies against the disease over time [12]. However, booster vaccination has been shown to be effective in preventing the onset of the disease and reducing the risk of severe disease [13-15]. Therefore, we consider it meaningful to assess COVID-19 antibody levels periodically after vaccination and booster shots to prevent such infections. We measured the antibody levels of our medical staff against COVID-19 monthly after COVID-19 vaccination and examined changes in antibody levels after administration of additional vaccination during a one-year period.
Materials and Methods
Subjects
The subject was a 64-year-old male medical staff of our corporation who received the COVID-19 vaccine by Pfizer-BioNTech twice and received an additional vaccine dose by Moderna eight months after the second vaccine dose and was administered COVID-19 antibody testing monthly for a year.
Ethical Principles
The present study was conducted in accordance with the Declaration of Helsinki, and the Seikokai Group Ethics Committee approved the study protocol. Informed consent was obtained from the staff.
Methods
The staff member received two doses of the COVID-19 vaccine by Pfizer-BioNTech between 10 June and 1 July 2021 and was subsequently administered COVID-19 antibody testing over time. Following that, he received an additional booster COVID-19 vaccine by Moderna on 21 February 2022 and was subsequently administered COVID-19 antibody testing over time. Antibody levels were measured monthly: one month after the completion of the second vaccination [16], two months after the second vaccination, and three months after the second vaccination. Subsequently, the fourth, fifth, and sixth measurements were performed every one month. An additional vaccine dose was administered eight months after the second vaccination. The seventh antibody level was measured one month after the additional vaccine dose, and the eighth, ninth, and tenth measurements were performed every one month, respectively. In total, the fluctuation of antibody levels was monitored for a year. Antibody levels were measured by quantification of spike protein-specific IgG antibodies, which have neutralizing activity against the receptor-binding domain of the virus. Abbott SARS-CoV-2 IgG (Abbott Japan, Minato-ku, Tokyo, Japan; cutoff value: 50 AU/mL) was used to perform this measurement.
Results
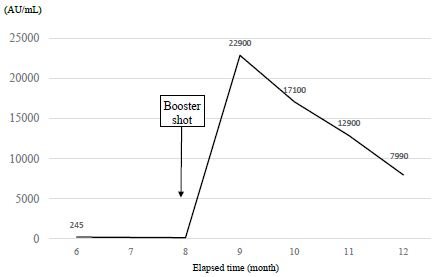
The time course of the antibody levels after two doses of the vaccine for the first 6 months is shown in Figure 1. The antibody level at one month after the second vaccine dose was 3,337 AU/mL, but that at the next month was 1,510 AU/mL, which is a decrease of 55%. The antibody level at three months after the vaccination was 749 AU/mL, a 78% decrease from that at the first measurement. Antibody levels at 4, 5, and 6 months after treatment were 455, 287, and 245 AU/mL, respectively. The decline in antibody levels was relatively slow compared with that in the first three months (Figure 1: arrows). The time course of the antibody levels from six months to 12 months after two doses of the vaccine is shown in Figure 2. After the administration of booster vaccine dose, the antibody level was remarkably increased to 22,900 AU/mL (at 9 months) and declined to 17,100 AU/mL (at 10 months), 12,900 AU/mL (at 11 months), and 7,990 AU/ml (at 12 months). However, the antibody level after the additional vaccine dose was relatively higher than that after the second dose. The total course of vaccination and antibody levels for a year period are shown in Figure 3.
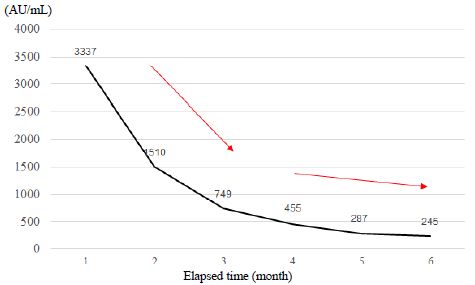
Figure 1: Time course of the antibody levels for six months after administration of a second vaccine dose
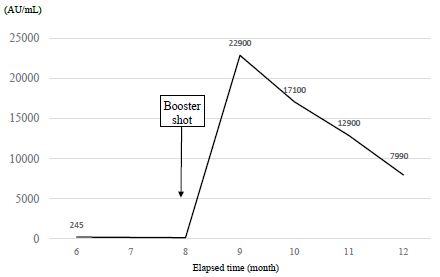
Figure 2: Changes in the antibody levels after administered an additional vaccine dose
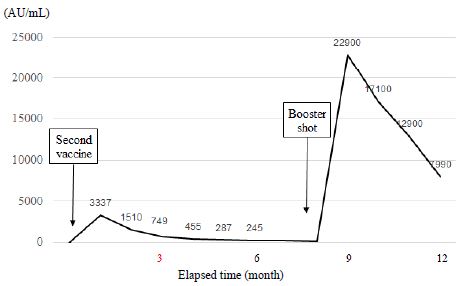
Figure 3: Total time course of vaccine doses and antibody tests for a-year period
Discussion
How antibody levels change after COVID-19 vaccine dose is now a matter of concern not only for healthcare professionals but also for the general population. In this study, we evaluated the antibody levels of our medical staff following vaccination and booster shot for COVID-19 every month during a one-year period. After two doses of the vaccine, the antibody level at three months decreased by 78% from baseline and at six months, decreased by 93% from baseline. This result indicates that the degree of decrease in antibody levels in the first three months was higher than that in the second three months, and the current results support our previous study [17]. We also demonstrated that after the administration of the booster shot, the antibody levels were remarkably increased and significantly higher than that after the second vaccine dose (Figure 3). Notably, the antibody levels remained high even after several months of the booster shot. Our current data also showed similar results to those of the previous studies [18-21]. It has been thought that the vaccinations increased at the same time as the outbreak of the delta strain that began in May last year from India [22-24], contributing to the convergence [25] of COVID-19 worldwide; however, the subsequent decrease in antibody levels may have contributed to the new omicron strain outbreak. However, the administration of additional doses of the vaccine is considered a significant countermeasure against COVID-19 because it was shown that the antibody levels against the disease increased again after the additional doses and that the severity and mortality rate from COVID-19 were reduced by the additional vaccine doses [26,27]. This remarkable increase in antibody levels after the additional vaccine dose may also contribute to the convergence of the omicron strain. We believe that the current data may help infection measures against COVID-19 for doctor, nurse, and other medical staff.
Study Limitations
The serum sample was obtained from one medical staff, and a large-sample investigation is needed to confirm our current study.
Conclusion
We measured the antibody levels of our medical staff over time after COVID-19 vaccination and examined changes in antibody levels after the administration of the booster vaccination for a year. Although the antibody levels declined with time after vaccination, we showed that the antibody levels significantly increased again after booster vaccination and remained high for several months.
Acknowledgment
The authors deeply indebted Saeki Ishiwata for providing serum samples and technical assistance for this research. The authors also thank to Bio Medical Laboratories Incorporated (BML, Inc.) for valuable support.
The preliminary data of this study was presented at a 4th European Congress on Infectious Diseases via live on 11 November 2022 at Paris, France, and on demand web streaming.
Funding
The authors declare that they have nothing to disclose regarding funding.
Conflict of Interest
The authors state that they have no conflict of interest to declare.
Author Contributions
Ikuma Kasuga conceived the work and designed the study protocol. Yuko Ishii contributed to the data curation and laboratory analysis. Yoshimi Yokoe and Osamu Ohtsubo supervised the project. Ikuma Kasuga contributed to the writing of the original draft, and all authors contributed to the revision of the manuscript and approved the final manuscript version.
References
DOI: 10.31038/CST.2023811
Abstract
Background and aim: Colorectal Cancer (CRC) is the third leading cause of global cancer death in humans and its incidence is gradually rising in developing nations including Bangladesh. The study was carried out to unveil the demographic and clinicopathological profile of CRC cases in Bangladeshi patients.
Methods: A cross-sectional study was conducted among purposively selected 50 patients irrespective of age and sex with histologically proven colorectal cancer at a tertiary level hospital for a period of 2 years. Large bowel resection specimens of CRC made the samples. Demographic and clinical information were recorded in a pre-tested, structured case record. Relevant macroscopic and microscopic features of tumors were recorded during gross and microscopic examinations of the specimen.
Results: Mean age of the CRC patients was 48.60±14.6 years. Adult active males (35-54 years old) were significantly affected by CRCs (p=0.0001). Per rectal bleeding (38.7%) and generalized weakness and pallor (38.98%) were the most frequent findings in distal and proximal CRCs, respectively. Adenocarcinoma NOS was the most commonly observed histologic type. Occurrence of CRC and tumour grades were significantly (p=0.0001) related where Grade-II and Grade-III tumour occurred in 72% and 24% of cases, respectively. Majority of the cases were presented at stage pT3 (68%) and pN0 (48%). Tumors in adult active age showed a higher tendency to be presented at advanced stages.
Conclusions: Bangladeshi adult active males of 35-54 years old were predominantly affected by a locally advanced stage of CRC. Routine screening programs are proposed for early detection and treatment of the cases.
Keywords
Colon cancer; Bangladeshi patients; Clinical features; Demographic characteristics; Intestinal tumor
Introduction
Colorectal cancer is one of the most common cancers globally. It is the second most common malignancy among women and the third most common malignancy in men [1]. The global burden of colorectal cancer is expected to increase by 60% by 2030. Its incidence shows a 10-fold variation across the world [2]. The prevalence of colorectal cancer is lower in Asia than in Western countries. But the incidence has been alarmingly increasing in countries of the Asia-Pacific region during the last two decades due to the westernization of lifestyles [3]. In Bangladesh, 5-year prevalence of colon and rectal cancer are 3.28 and 3.1 per 100,000 population, respectively [4]. There are variations in risk factors, mode of disease presentation, sub-site distribution, tumor morphology, grade and stage at presentation. These tumors grow insidiously and remain undetected for long periods remaining potentially curable, premalignant lesions over several years. Therefore, screening procedures provide a unique opportunity for cancer prevention [5]. However, in the long run, the tumor cells metastasize to lymph nodes and in the other organs. The treatment, prognosis and survival rate largely depend on the stage of disease at diagnosis.
The development of both familial and sporadic colorectal cancers can be influenced by genetic factors [6]. Age is another major risk factor for sporadic CRC. The diagnosis is rare before the age of 40 years. The incidence starts to increase significantly between 40 to 50 years and the age-specific incidence rates raise in each succeeding decade thereafter [7]. Although patients over 50 years of age represent 90% of newly diagnosed cases [8], the trend is changing with the increasing incidence among the younger population who present in a more advanced stage [9]. In recent years, tumor location has also been suggested to be a valuable predictor, which has added to the difficulty of discussing its clinicopathological features and outcomes [10]. The majority of colorectal cancers belong to classical adenocarcinomas, with several histological variants associated with specific molecular characteristics [11,12]. Understanding these features could guide the proper management and prognosis of the patient. But unfortunately, there is a scarcity of data regarding the demographic and clinicopathological patterns of colorectal cancers in Bangladeshi patients. Therefore, the present study was undertaken to understand the demographic and clinicopathological profiles of patients with colorectal carcinoma in Bangladesh.
Methods
Ethical Approval
This study was approved by the local Ethics Committee (Institutional Review Board) at Bangabandhu Sheikh Mujib Medical University (BSMMU) and informed consent was obtained from all participants.
Study Design, Period and Sample
This cross-sectional, descriptive, hospital based, study was conducted in the Department of Pathology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh during the period of March 2019 to February 2021. Large bowel resection specimen histologically diagnosed as adenocarcinoma at the department of Pathology, BSMMU were included in this study. A total of 50 primary colorectal carcinoma cases irrespective of ages and sexes were included in the study. Clinically suspected colorectal carcinoma subsequently proved to be non-epithelial tumors of the colon were excluded from this study. Patients’ attendants were interviewed for demographic and clinical information, which were recorded in a performed questionnaire.
Gross and Microscopic Evaluation of Samples
During gross examination tumor site and macroscopic features of tumors were noted. Splenic flexure was taken as demarcating point of proximal and distal lesions. After that representative tissue blocks were submitted for routine processing and paraffin embedding. Standard protocol was maintained during tissue processing and staining. Microscopic examination of tissue sections stained with hematoxylin and eosin was carried out and relevant points were recorded. The tumors were classified following World Health Organization classification of tumor and grading of tumor was done by using AJCC specified four-tiered grading system. Staging was performed following TNM Classification of Colorectal Carcinoma American Joint Committee on Cancer (AJCC).
Statistical Analysis
Data was entered in MS Excel and analyzed by using SPSS software version 21. Categorical variables were expressed as percentages and analyzed using the Chi-square test or Fisher’s exact test. Continuous variables were expressed as mean or median and analyzed using the Mann-Whitney test. Demographic factors and clinical characteristics were summarized with percentages for categorical variables and median for continuous variables.
Results
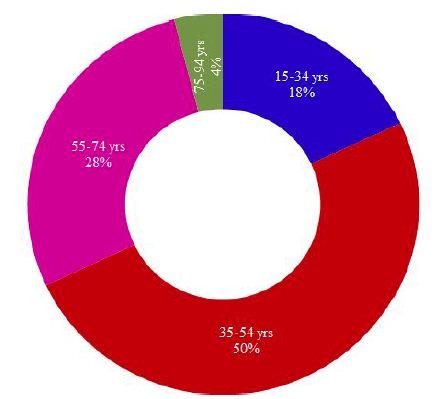
A total of 50 patients with CRC were enrolled in this study. Age of the study population varied from 19-85 years with a mean of 48.60±14.6 (SD) years. All the 50 cases were categorized into four age groups where samples from patients belonging to 15-34 years, 35-54 years, 55-74 years and 75-94 years were considered as young, adult, elderly and old age groups, respectively. Figure 1 illustrates the distribution of CRC cases in different age groups.
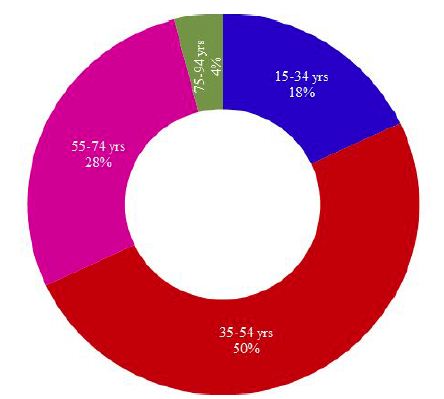
Figure 1: Distribution of CRC cases in different age groups of Bangladeshi patients
As shown in Figure 1; half (50%) of the CRC cases belonged to adult active age group (35-54 years), followed by 28% cases in elderly (55-74 years), 18% cases in young (15-34 years) and 4% cases in old age group (75-94 years). A chi-square test of independence was performed to examine the relationship between age groups and the frequency of occurrence of CRCs. The relation between these variables was significant, X2 (3, N=50)=22.48, p=.0001 at α=0.05. The adult active age group (35-54 years) was more likely to be affected by colorectal carcinoma than the other groups.
Sex-wise distribution of CRC cases of this study revealed that almost two-thirds (64%) of the study cases were male while around one-third (36%) cases were female. The occurrence of male cases was numerically high in all age groups except the old age where the percentage of both cases was equal (Figure 2). The relation between the occurrence of CRS and sexes was weakly significant, [X2 (1, N=50)=3.92, p=.048 at α=0.05]. Males were more likely to be affected by colorectal carcinoma than females (Figure 2).
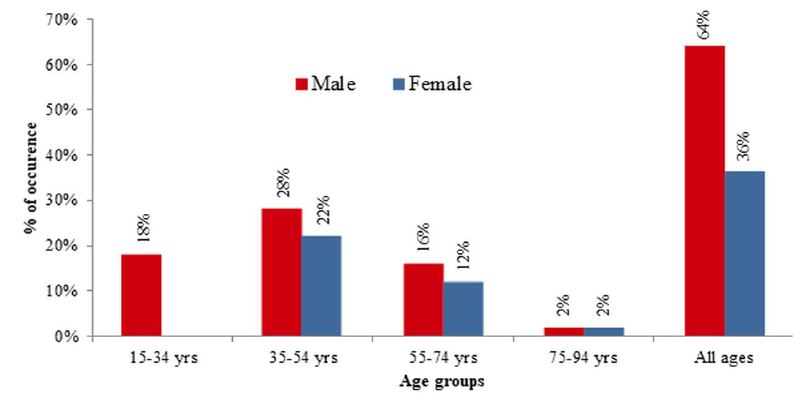
Figure 2: Sex-wise distribution of CRC cases in different age groups of Bangladeshi patients
Per rectal bleeding was the most frequent clinical presentation of CRC among the study population that was documented in 30% of cases followed by generalized weakness and pallor (26%), abdominal pain with or without features of obstruction (16%), altered bowel habit (12%), weight loss (12%) and abdominal mass (4%). Only one study case had a positive family history of colon cancer. None of the cases was presented with a history of extra-colonic malignancy. When the site of occurrence was considered, the tumor was located in the distal colon and proximal colon in 62% and 36% of cases, respectively. Only one (2%) of cases were recorded to have synchronous tumors involving both colons. However, no signification relation was observed between the tumor sites and the occurrence of CRC [X2 (1, N=50)=2.880, p=.090 at α=0.05]. The distribution of study cases based on tumor location along with presenting complaints is shown in Table 1.
Table 1: Distribution of study cases based on tumor location along with presenting complaints
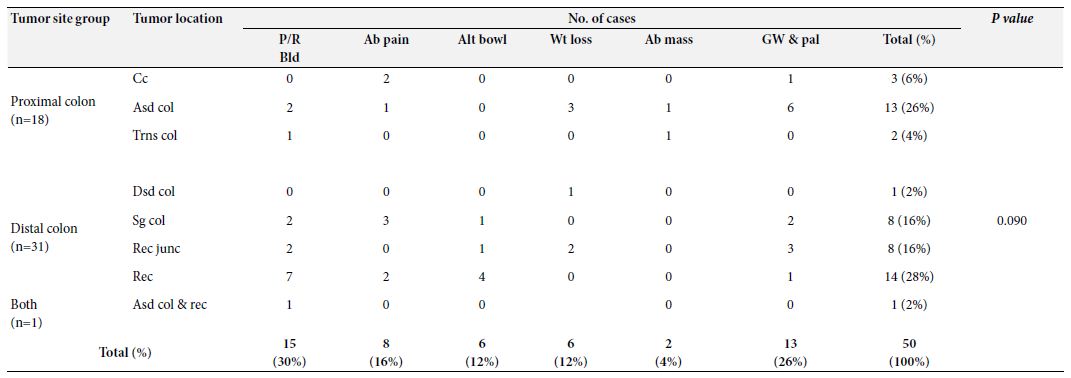
P/R Bld: Per rectal bleeding; Ab Pain: Abdominal pain; Alt bowl: Altered bowel habit; Wt loss: Weight loss; Ab mass: Abdominal mass; Gw & pal: Generalized weakness and pallor; Cc: Cecum; Asd. col: Ascending colon; Trns col: Transverse colon; Dsd col: Descending colon; Sg col: Sigmoid colon; Rec junc: Rectosigmoid junction; Rec: Rectum: Asd. col. & rec.: Ascending colon & rectum (synchronous)
The exophytic pattern was the most common gross morphology which was observed in more than half (60%) of the cases, followed by ulcerating and infiltrative patterns, seen in 30% and 10% of the cases, respectively. In our study, the frequency of the Exophytic pattern was significantly higher than the other two patterns based on the chi- square test of independence, [X2 (2, N=50)=19.00, p=.0001 at α=0.05] indicating that Exophytic pattern was more likely to occur in CRC cases (Table 2).
Table 2: Distribution of study cases based on tumor morphologies
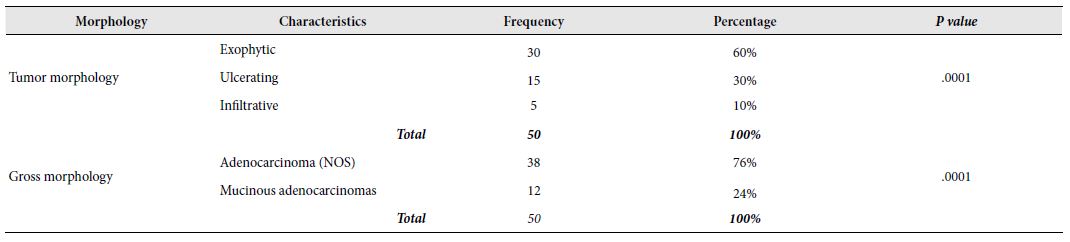
In this study, only two variants of adenocarcinoma were observed; the commonest one being adenocarcinoma (NOS) (76%) followed by mucinous adenocarcinomas (24%). The frequency of adenocarcinoma (NOS) in relation to CRC cases was highly significant [X2 (1, N=50)=13.52, p=.0001 at α=0.05] compared to mucinous adenocarcinoma. It seemed that adenocarcinoma (NOS) was the more frequent variant of CRC in Bangladeshi patients (Table 2). Among the 50 selected cases, majority (72%) of the tumours belonged to grade II (moderately differentiated) tumors. Remaining 24% and 4% cases were categorized as grade III (poorly differentiated) and grade I (well differentiated) tumors, respectively. There was a highly significant relation between the occurrence of CRC the and grade of tumours [X2 (2, N=50)=36.640, p=0.000 at α=0.05]. However, no significant relationship was seen between the tumour grades and age groups [X2 (6, N=50)=2.702, p=0.845 at α=0.05] or sex [X2 (2, N=50)=1.292, p=0.524 at α=0.05]. It seemed that Grade-II CRCs were more likely to occur in case of colorectal carcinoma in Bangladeshi patients irrespective of age and sex. Figure 3 illustrates the graphical presentation of grades of tumours according to age groups and sexes whereas Table 3 summarizes the frequency of tumours according to grades, age groups and sexes with their relationship.
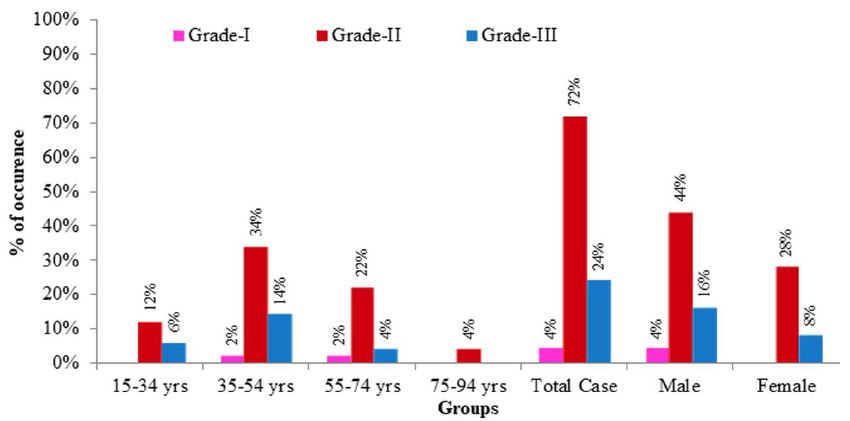
Figure 3: Graphical presentation of grades of CRC cases according to age groups and sexes. Grade-I: well differentiated tumors; Grade-II: moderately differentiated tumours; Grade-III: poorly differentiated tumours.
Table 3: Frequency of tumours according to grades, age groups and sexes with their relationship
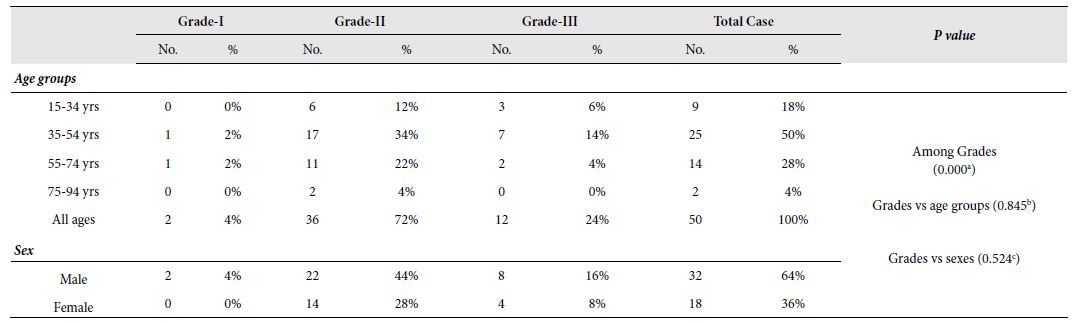
No.: Number of occurrence; %: Percentage of occurrence;
a: X2 (2, N = 50) = 36.640, p = 0.000 at α = 0.05; b: X2 (6, N = 50) = 2.702, p = 0.845 at α = 0.05; c: X2 (2, N = 50) = 1.292, p = 0.524 at α = 0.05
According to the pathological depth of invasion, studied CRC cases were ranked into 4 stages namely PT-I, PT-II, PT-III and PT- IV starting from lowest to highest invasion. Stage-3 (PT-III) was the most commonly recorded stage of tumour which was seen in 68% of the cases followed by PT-II, PT-IV and PT-I which were recorded in 22%, 8% and 2% cases, respectively. A highly significant relation was observed between the occurrence of CRC and the stage of tumours based on pathological invasion [X2 (2, N=50)=36.640, p=0.000 at α=0.05]. It seemed that PT-III is more likely to occur in Bangladeshi CRC cases. A highly significant relation was also observed between the pathological invasion of tumours and age groups [X2 (6, N=50)=2.702, p=0.845 at α=0.05] where adults are more likely to be affected by Stage-3 (PT-III) CRCs. However, no significant relationship was seen between the tumour stages and sex [X2 (2, N=50)=1.292, p=0.524 at α=0.05]. A graphical presentation of stage of tumours according to age groups and sexes has been depicted in Figure 4 and the summary of the frequency of tumours according to stages, age groups and sexes with their relationship is shown in Table 4.
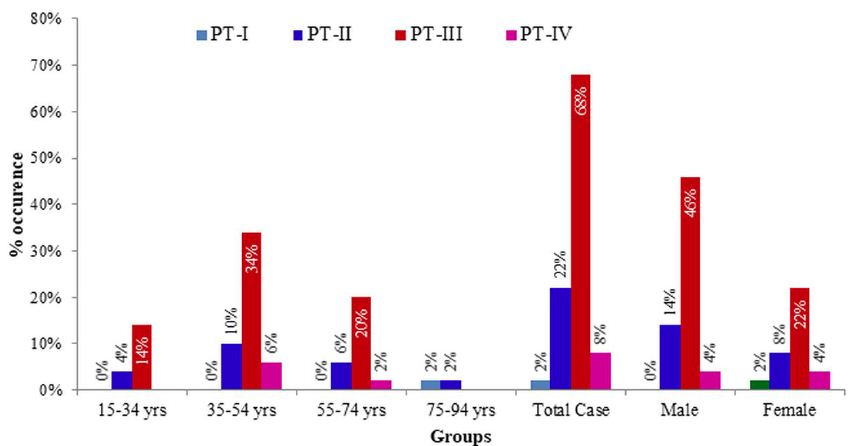
Figure 4: Graphical presentation of stages of tumours according to age groups and sexes. PT-I: low pathological invasion; PT-II: moderate pathological invasion, PT-III: fair pathological invasion; PT-IV: high pathological invasion.
Table 4: Frequency of tumours according to stage of tumor based on the pathological depth of invasion. age groups and sexes with their relationship.
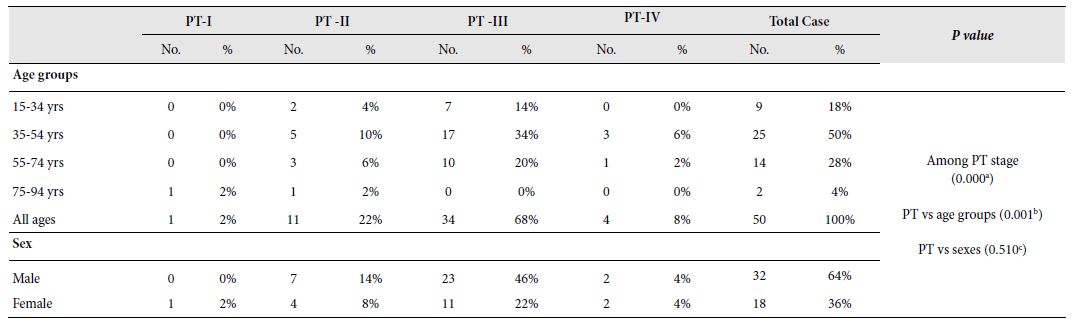
PT-I; PT-II; PT-III; PT-IV; No.: Number of occurrence; %: Percentage of occurrence;
a: X2 (2, N = 50) = 36.640, p = 0.000 at α = 0.05; b: X2 (6, N = 50) = 2.702, p = 0.845 at α = 0.05; c: X2 (2, N = 50) = 1.292, p = 0.524 at α = 0.05
Studied CRC cases were further classified based on the involvement of regional lymph nodes by the tumor (PN) where cases with no lymph node involvement was grouped in PN0, metastasis in one to three regional lymph nodes in PN1, metastasis in four or more regional lymph nodes in PN2 and the cases where Lymph nodes could not be assessed was grouped in PNx. Almost half (48%) of the study cases was categorized in PN0 followed by PN2, PN1 and PNx in 26%, 22% and 4% cases, respectively. The involvement of regional lymph nodes was highly related to the occurrence of CRCs [X2 (3, N=50)=19.600, p=0.000 at α=0.05]. It is more likely that regional lymph nodes were not involved in CRC cases. However, no significant relationship was seen between the lymph node invasion and age groups [X2 (9, N=50)=6.915, p=0.646 at α=0.05] or sex [X2 (3, N=50)=2.620, p=0.454 at α=0.05]. Figure 5 illustrates the graphical presentation of different classes of CRC cases based on the involvement of regional lymph nodes according to age groups and sexes whereas Table 5 summarizes the frequency of different classes of CRC cases based on the involvement of regional lymph nodes according to stages, age groups and sexes with their relationship.
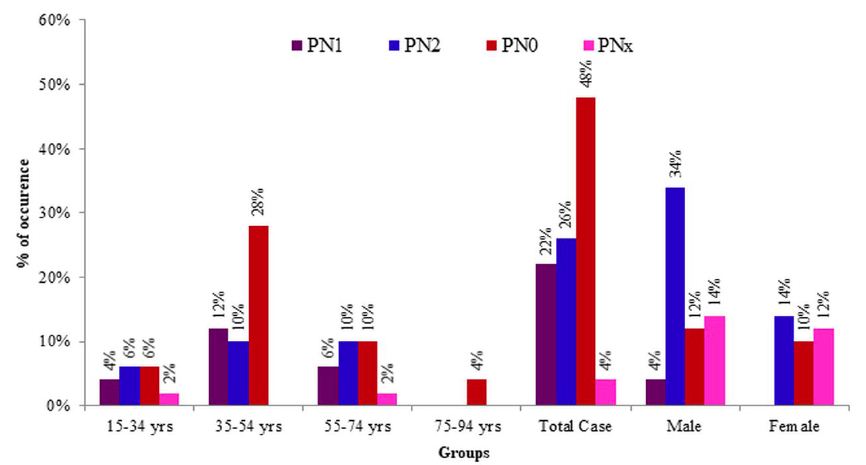
Figure 5: Graphical presentation of different classes of tumours based on involvement of regional lymph nodes according to age groups and sexes. PNO: no lymph node involvement; PN1: metastasis in one to three regional lymph nodes; PN2: metastasis in four or more regional lymph nodes; PNx: lymph nodes could not be assessed.
Table 5: Frequency of tumours according to involvement of regional lymph nodes by the tumor, age groups and sexes with their relationship
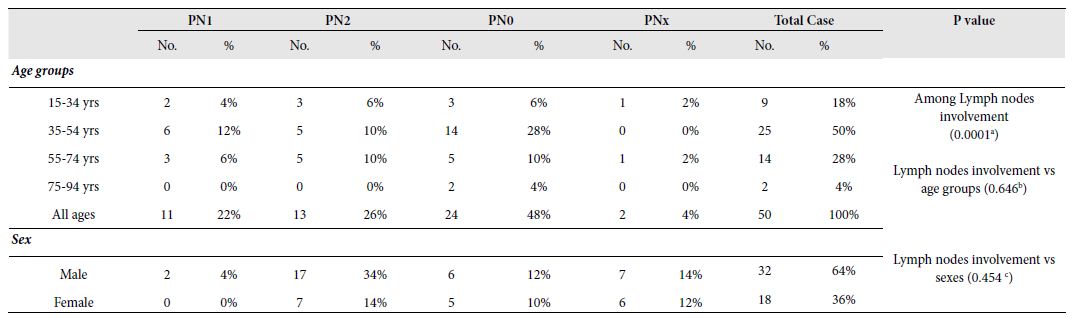
N1: ; N2: ; N3: ; N0: ; No.: Number of occurrence; %: Percentage of occurrence;
a: X2 (3, N = 50) = 19.600, p = 0.0001 at α = 0.05; b: X2 (9, N = 50) = 6.915, p = 0.646 at α = 0.05; c: X2 (3, N = 50) = 2.620, p = 0.454 at α = 0.05
Discussion
Although CRC is more likely to occur at old age, nowadays, younger patients are increasingly affected by different types of CRCs [13]. In this study, half (50%) of the cases belonged to the 35-54-years age group, with a mean of 48.60 ± 14.6 years which is lower than that reported age from the Western world [13-15]. Salminen, et al., 2005 recorded 59 years as the mean age of CRC in their study in the Finnish population and Turner, 2014 observed only 20% cases to occur below the age of 50 years [14,15]. However, Saha et al., 2016 and Raza et al., 2016 recorded the mean age as 50.77 years and 47 ± 14.8 years, respectively in Bangladeshi colorectal cancer patients [16,17], which are in good agreement with this study. The occurrence of CRCs specially in relatively young age group may be attributed to the recent change in food habits of Bangladeshi active-aged people (35-54 years) who have shifted to western diets that ae well documented as a contributor to colon cancer. It has been reported that consumption of red or processed meats is associated with an increased risk of colon cancer [18]. Consumption of high fat containing foods like red or processed meats induces increased bile acids secretion that in turn results in altered microbial composition in gut [19, 20]. Such alternation in microbial community contributes to the production of different metabolites that might influence the development of colon cancer [20]. Moreover, geographical and environmental factors of the study population may have influenced the findings as well. However, the higher incidence of CRCs in the younger age group of Bangladeshi patients in comparison to western studies is alarming. This interesting finding necessitates the importance of cancer screening program and this report may be considered in future studies to evaluate predisposing and genetic factors for CRCs in this region.
In the current study, there was male preponderance (64%) with a male to female ratio 1.8:1. Studies conducted elsewhere also showed higher incidence of CRC among male patients [14,16,17]. Urbanization and changes in lifestyles might have contributed to the transformation in food habit from native to western diets rich in high fat which are known to trigger colon cancer. In association with altered food habit, higher incidence of smoking, alcohol consumption or genetic factors might be responsible for this male predominance.
Clinical presentations are different for proximal and distal CRC. In our study, per rectal bleeding was the most frequent finding (38.7%) in distal CRCs whereas, generalized weakness and pallor were the chief complaints of the patients with CRCs in proximal colon (38.98%). These features are consistent with the findings of reported elsewhere [5].
The most commonly observed location of CRC in this study is distal colon (62%). Rectum was most frequently observed site (28%). Other Bangladeshi studies conducted also found similar findings [17,21,22]. Occurrence of CRC in Bangladeshi population is higher in distal colon due to some unknown etiology which may be related to some genetic factors.
The exophytic pattern was the most common gross morphology observed in 60% cases followed by ulcerating (30%) and infiltrative pattern (10%). In this study, only two histological types of colorectal adenocarcinoma: adenocarcinoma (NOS) and mucinous adenocarcinoma were observed. Adenocarcinoma (NOS) comprises the majority (76%) of the total cases. These findings were consistent with the findings of other studies indicating common gross and histopathological feature of CRCs [17,21-23].
Among the 50 cases, 72% cases were Grade II tumours, 24% were Grade III and 4% were Grade I tumours. All of the mucinous adenocarcinoma was considered poorly differentiated (grade III). Several studies suggest that CRCs occuring in younger patients (less than 50 years of age) are less differentiated [24]. In the present study, 34% of Grade-II and 14% of Grade III tumours were observed in 35- 54 years of age whereas 22% Grade-II and 4% Grade III tumours were recorded in 55-74 years of age. Present study findings are in close agreement with previous findings that documented less differentiated CRCs are likely to occur within 50 years of age [23]. However, a statistically significant association between age group and tumor grade was not observed possibly due to a smaller sample size.
We also categorized study cases according to the PT and PN stage of the tumor. Our study revealed that PT3 (68%) and PN0 (48%) were the most commonly reported stages of tumor in CRC cases based on the depth of invasion and lymph node metastasis, respectively. Studies conducted elsewhere reported that colorectal cancers in young patients (<50 years of age) are biologically aggressive and present at advanced stage [9,25]. In our study, PT3 and PT4 stages were recorded in 34% and 6% cases, respectively in 35-54 years age group in comparison to 20% PT3 and 2% PT4 stages in 55-74 years age group. In the case of nodal staging, metastasis in one to three regional lymph nodes (PN1) was observed in 12% of cases in 35-54 years age group which was double of the observed cases (6%) in the 55-74 years age group. Our study findings for pathological invasion and metastasis in lymph nodes in CRC cases clearly support previous study reports that documented biological aggressiveness and advanced stage in colorectal cancers in patients under 50 years of age. All these studies suggest that patients with colorectal adenocarcinomas usually present with advanced morphology in histopathology.
Conclusion
Present study findings on colon cancer were different from that described in the western countries. Active aged people (35-54 years old) were found to be significantly affected by CRC in our study. In majority of the cases, the tumour presented at a locally advanced stage. Quick urbanization, fast shifting to western food, lack of proper knowledge on CRC might account for some of these differences. Routine screening program is proposed for early detection and treatment of the cases to reduce the burden of morbidity and mortality. Genetic tests should also be carried out to unveil the cause of young age presentation of CRCs. However, this study had its own limitations. The study reflects to the findings of a specific geographical area with a small sample size. Therefore, further studies should be conducted all over the country with a larger sample size for a more comprehensive understanding on demographic and clinicopathological profiles of CRCs in Bangladesh.
Acknowledgements
The authors gratefully acknowledge the logistics and grant support to conduct the research activities from Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh.
Availability of Data and Materials
Raw data, supplemental data and materials are available on request.
Conflict of Interests
The authors declare that they have no conflict of interests in publishing the article.
Ethical Consideration
Written consent from individual patient/representative of patients was obtained for using the samples for research purposes. No personal data/information of patients was shared in public.
Author’s Contributions
SSUM planned, designed and performed the study. She also wrote the manuscript (MS). FB, MMR & AZ helped in planning & designing of the study and developing the research question. PR, TI, USS, UTN, SA and NA helped in data collection and processing. KBMS helped in study design, data screening and performed data analyses, interpretation and MS writing. All authors read and approved the final manuscript.
References
Abstract
Introduction: Bilateral optic neuropathy caused by the novel coronavirus SARS-CoV2 (COVID-19).
Case report: A 25 years old female COVID-19 (+) applied to our clinic with complaints of bilateral progressive visual loss. Two weeks prior to onset of eye and vision symptoms, she had tested positive for coronavirus disease (COVID-19) virus by nasopharyngeal polymerase chain reaction (PCR) after developing symptoms of shortness of breath and cough. One week prior to her admission, bilateral blurred and vision loss progresivvely. In her ophthalmological examination; right and left visual aquity were 10/200 with blurred vision and ocular tensions were 15 mmHg and 16 mmHg, right and left, respectively. Anterior segment in both eyes were natural, there were no active cells, however, there were optic disc edema and retinal edema in both eyes. The diffusion cranial MR was normal.
Discussion: Optic neuropathies is a clinical diagnosis based on the history and examination findings, generally. Because important findings on funduscopic examination help differentiate typical from atypical cases of optic neuritis, an ophthalmologic examination can be considered in the clinical evaluation. Our patient is believed to have acute bilateral optic neuropathies induced by COVID-19 infection. Ispite of optic neuropathies in young ages are usually associated with MS, our patient is an interesting and rare case induced by COVID-19 infection with bilateral optic neuropathies.
Keywords
The novel coronavirus SARS-CoV2 (COVID-19), Optic neuropathy
Introduction
Optic neuropathies in adults are usually unilateral and commonly linked to multiple sclerosis (MS). It usually occurs as sudden onset of visual loss associated with pain on eye movement and progress in its course to reach its maximum deficit in a week [1]. Diagnosis is usually clinical based on history and examination findings. Brain and orbital imaging such as magnetic resonance imaging (MRI) help in the diagnosis in most cases. After confirmation, treatment is usually standart. Bilateral acute optic neuropathies are seen rarely, particularly in individuals without known systemic inflammatory or autoimmune disorders.
Case Presentation
A 25 years old female COVID-19 (+) (the novel coronavirus SARS-CoV2) patient came to our clinic with bilateral vision loss in august 2021. Two weeks prior to onset of eye and vision symptoms, she had tested positive for coronavirus disease (COVID-19) virus by nasopharyngeal polymerase chain reaction (PCR) after developing symptoms of shortness of breath and cough. She was quarantined at her home and treated symptomatically with improvement; she never required hospitalization for his respiratory illness nor medications including hydroxychloroquine.
One week prior to her admission, bilateral blurred and vision loss progresivvely. She has no past medical history presented from clinic with bilateral eye pain and vision loss and family history of any neurological or immunological diseases. In her ophthalmological examination; right and left visual aquity were 10/200 with blurred vision and ocular tensions were 15 mmHg and 16 mmHg, right and left, respectively. Anterior segment in both eyes were natural, there were no active cells, however, there were optic disc edema and retinal edema in both eyes (Figures 1 and 2), and also seen in optic coherence tomography (OCT) (Figures 3 and 4). The diffusion cranial MR was normal.
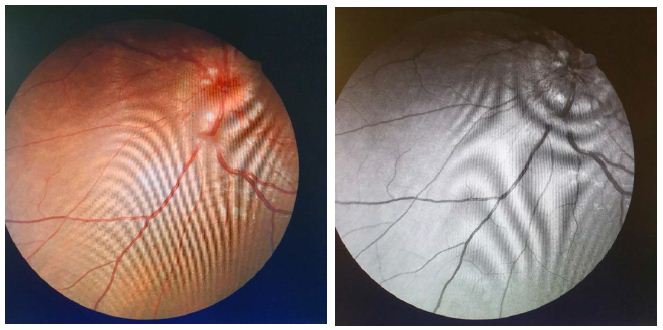
Figure 1: Right eye fundus photography
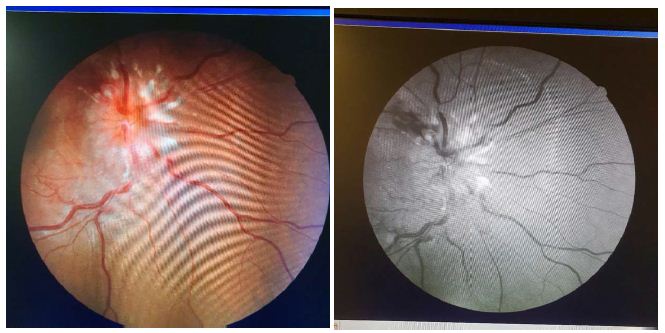
Figure 2: Left eye fundus photography
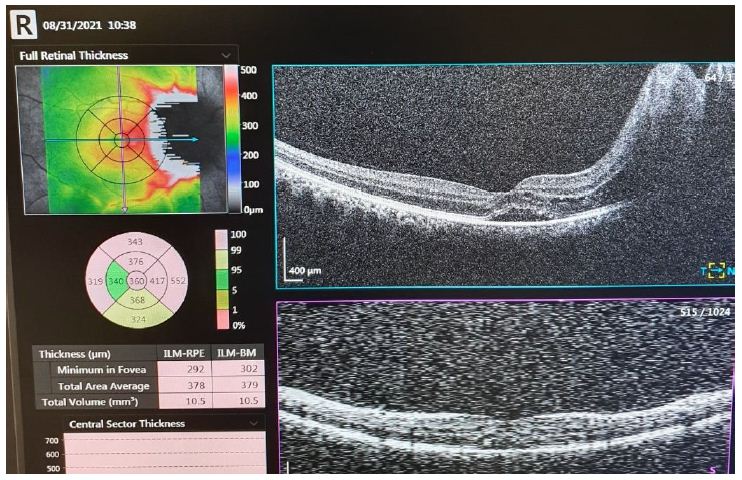
Figure 3: Optic coherence tomography of right eye
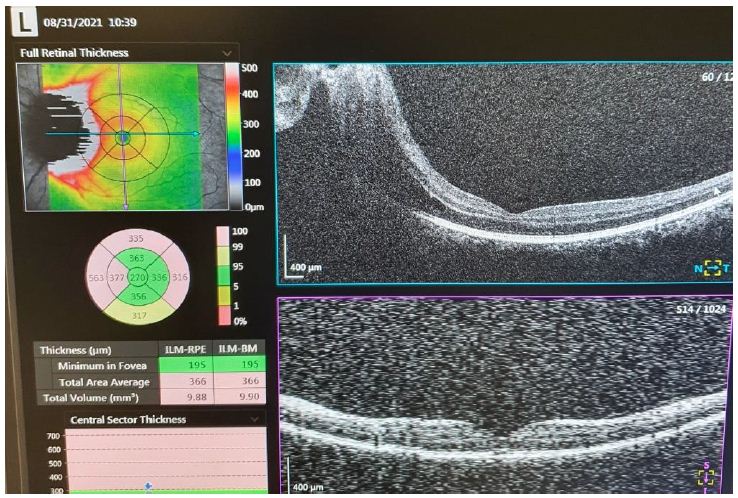
Figure 4: Optic coherence tomography of left eye
Our patient was started on methylprednisolone 1 g every 24 hours for a total of 5 days/doses. Within 48 hours, his vision and eye pain had shown significant improvement. By day of discharge, our patient had complete restoration of vision in the left eye with remarkable but not complete vision recovery in the right eye. He was discharged on a tapering dose of prednisone over 4 weeks with planned follow-up with ophthalmology and neurology.
Discussion
Optic neuropathy is defined as a demyelinating, inflammatory condition that causes acute, usually monocular, visual loss. It is highly associated with MS, and it is the presenting feature in 15% to 20% of these patients and occurs in 50% of them at some time during their illness [2].
It is believed that the demyelination in optic neuropathies is immune-mediated, but the exact targeted antigens remain unknown [3].
Optic neuropathies is a clinical diagnosis based on the history and examination findings, generally. Because important findings on funduscopic examination help differentiate typical from atypical cases of optic neuritis, an ophthalmologic examination can be considered in the clinical evaluation. MRI of the brain and orbits with gadolinium contrast provide a better assessment of the diagnosis in most cases. Further diagnostic testing, such as lumbar puncture, is done to exclude other causes of visual loss in atypical cases. However, around 60% to 80% of patients with acute optic neuropathies have nonspecific findings in the CSF such as lymphocytes and elevated proteins [4].
Our patient is believed to have acute bilateral optic neuropathies induced by COVID-19 infection. Once the diagnosis of optic neuropathies is made, treatment is usually straightforward with intravenous methylprednisolone (typically 1 g per day for 3 days) often followed by oral prednisone (1 mg per kg per day for 11 days), with subsequent tapering over a period of 4 days [2]. Treatment is associated with a more rapid recovery of vision by 2 to 3 weeks with no impact on long-term visual function. Therefore, a follow-up with neurology and ophthalmology after discharge is recommended to reach a final diagnosis in cases like this.
Ispite of optic neuropathies in these young ages are usually associated with MS, our patient is an interesting and rare case induced by COVID-19 infection with bilateral optic neuropathies.
Conclusion
Our patient described in this clinical vignette has signs and symptoms typical of acute bilateral demyelinating optic neuritis on his presentation. His evaluation with brain and orbital MRI along with lumbar puncture to determine the possibility of MS or other autoimmune disease was negative as well as other laboratory assessment. Therefore, we believe his infection with COVID-19 virus has triggered his immune system to present these findings. COVID-19 virus infection is causing a huge impact in the world as pandemic; its extent as clinical disease is still poorly understood and explained.
Declaration of Interest
I have no declaration of interest.
References
Abstract
The reasons for the misconceptions that have arisen in modern ideas about the features of acute nonseptic inflammation of the lung tissue and the direction od necessary correction are considered.
Keywords
Acute pneumonia, Etiology, Pathogenesis, Disease doctrine
Acute inflammation of the lung tissue or acute pneumonia (AP) is one of the oldest medical nosologies, which has been and remains one of the most serious diseases. Despite the severe nature of clinical manifestations, this disease has never had any reason to consider it dangerous from an epidemiological point of view.
For most of the history of the AP, the lack of sufficient scientific information about the features of the disease did not allow purposefully substantiating the most optimal means of medical care. Therefore, the search and selection of effective methods of treatment took place empirically, by trial and error. Nevertheless, such an intuitive search for medical care for these patients allowed ancient medicine to identify methods that were subsequently used with sufficient success for many centuries until the last decades. In this case, we are talking primarily about first aid methods, the timely use of which could bring relief to the patient and reduce the severity of the disease. In different regions of the world, to achieve this effect, preference was given to such methods of care as cupping therapy, bloodletting or short-term cooling of the patient’s body. The evaluation of the results was purely subjective on the part of both doctors and patients. Therefore, if these methods did not bring the expected satisfaction, they could hardly remain in demand for thousands of years. The situation in this field of medicine began to change dramatically after the discovery and the beginning of the clinical use of antibiotics in the middle of the last century. By this time, medical science had information and facts that created prerequisites for the distortion of scientific views on the problem of AP under the influence of a new type of therapy.
The development of microbiology made it possible to identify the pathogens of AP, among which Streptococcus pneumoniae, discovered in the 19th century and given its name in this regard, played a dominant role. At the same time, this circumstance did not change the indifferent view of the epidemiology of the disease due to the absence of cases of the spread of AP in contact with such patients. Pneumococcus continued to consistently dominate among the pathogens of AP, and its frequency on the eve of clinical use of antibiotics continued to reach 90-95% [1-3]. Nevertheless, these processes were fairly interpreted as acute nonspecific inflammation, which emphasized the polymicrobial nature of its etiology.
Continuing to consider AP as an inflammatory rather than an infectious process, medicine was initially aware of the fact that antibiotics are able to act only against the microbial factor and do not have a direct effect on the mechanisms of inflammatory tissue transformation. However, the initial results of the use of antibiotics created the illusion that a universal remedy for the treatment of inflammatory diseases has been found. At the same time, the fact was overlooked that the successful suppression of the pathogens of the process required the patient’s body to independently eliminate the pathological deviations that had arisen, not only morphological, but also functional. In the resulting atmosphere of euphoria, the centuries-old experience of medicine remained unclaimed as a relic of the past, and the standard treatment of AP after a short period of time began to appear under the term “antibiotics alone”. The revision of the principles of AP treatment has led to equally radical changes in the didactics of medical personnel training. Therefore, when the side effects of antibiotics began to intensify, requiring the correction of unforeseen situations, efforts were made in the hope of reviving the previous effect of antimicrobial therapy. By now, persistent attempts to revive the etiotropic principles of AP treatment have become a strategic goal of solving the problem, and the process of deformation of ideas about its essence has gone so far that many indisputable facts that contradict the currently dominant concept of the disease have ceased to be the subject of discussion. The generally recognized fact of the emergence of a large group of antibiotic-resistant strains and the loss by antibiotics of their role as the leading therapeutic agent in AP is just the tip of the iceberg.
In recent decades, many experts have expressed concern about the growing role of viruses in the etiology of lung inflammation, which accounted for almost half of all AP diseases in the world about two decades ago [4-6]. The former relatively stable list of AP pathogens began to differ by changing priorities with periodic change of leaders. The initial prevalence of pneumococcus in the etiology of the disease in recent years has decreased to 10.9% – 22.5% among the positive results of a bacteriological study [7]. It would seem that in the presence of these circumstances, there is an obligatory need for a radical revision of views on this problem and a change in therapeutic principles. However, the realization of these obvious needs has not been observed in recent decades, and even during the SARS-CoV-2 pandemic, antibiotics unable to suppress the coronavirus continued to be presented as the main method of treating COVID-19 pneumonia [8-10]. The fear of coronavirus that arose during the SARS-CoV-2 pandemic and the transition to strict epidemiological measures were dictated not only by the appearance of a pathogen that is not quite familiar to the human body, but, above all, by the lack of effective ways to provide assistance. At the same time, the statistics of this unexpected event convincingly show that 80% of the infected population safely endured this incident on an outpatient basis without any specific medical care, and 20% of them learned about the presence of infection only by the results of the tests carried out [11,12].
These data only confirm the ancient postulate that people get sick with pneumonia, not infected. Inflammation of the lung tissue, which is not a fatal inevitability even during the last coronavirus pandemic, further revealed pressing problems with the principles of its treatment when such patients began to concentrate in specialized departments, which had a strong psychological impact on medical personnel [13,14]. The loss of the former effectiveness of antibiotics every year more and more acutely required additional methods of treatment. The interpretation of the need for such care in patients with AP and the choice of additional methods were completely based on the “microbial” concept of lung inflammation, which was formed during the use of antibiotics and considers microbiological factors as the main cause of the disease and its consequences. As a result of such a narrow definition of the main difficulties in the treatment of AP, the disease itself has been classified as infectious in recent years, although the sanitary and epidemiological conditions have remained the same. In addition, in recent years, the number of cases with septic complications of AP has begun to grow, but, unlike sepsis in other localizations of inflammation, it is in this group of patients that the bacteriological blood test often turns out to be negative [15,16].
Such a selective discrepancy between the diagnosis and the criteria for its confirmation for this category of patients receives truly striking explanations as a consequence of preliminary antibacterial therapy [15,17,18]. In other words, in accordance with the dominant concept of the leading role of the etiology of the process, it is assumed that successful antibacterial therapy eliminates pathogenic microorganisms, but, at the same time, does not save (!?) from generalization of infection. In recent years, the process of diagnosing septic complications has also emerged solely on the basis of analogies and without any convincing arguments in the case of viral forms of inflammation [16,19,20]. Even more puzzling are the principles of septic shock diagnosis in patients with AP, in whom the presence of the pathogen in the bloodstream barely exceeds 10% and in fact does not differ from this indicator in sepsis [21], but the level of peripheral blood pressure continues to be one of the leading criteria for this assessment. At the same time, the fact that the primary focus of the disease damages the vessels of the small circulatory circle, which have diametrically opposite indicators with the periphery and have a regulating effect on the overall blood flow, is completely ignored [22-24].
The prevailing ideas about septic complications in patients with AP today suggest the use of additional treatment methods that were previously justified and tested for other localizations of inflammation. The basis of such assistance is infusion-bolus therapy, the effect of which is directly opposite to the methods of old medicine, since it is accompanied by an additional load on the blood vessels in the area of lung damage. And since the effectiveness of these efforts leaves much to be desired, modern recommendations provide in advance for the subsequent administration of vasopressors [16-19].
As a result, modern medicine cannot achieve noticeable success in the treatment of the most severe forms of AP, in which mortality in intensive care units remains unprecedentedly high, reaching, according to some data, 91% [25]. At the same time, only some authors publish frank confessions that the condition of many patients from this group continues to deteriorate after the start of inpatient treatment and despite this [19], and the overwhelming number of patients with septic shock did not have it during hospitalization (!) and it developed already during treatment [26]. The prevailing ideas about pneumonia today are the reason for the intensified search for etiotropic treatment of these diseases in the hope of a revival of success comparable to the beginning of the era of antibiotics. However, the nonspecific nature of this nosology, combined with the constant change of leading pathogens, as well as the accumulated experience and profound biological consequences of the use of antibiotics create real doubts about such a revival. At the same time, viral pneumonia does not have a special treatment, and studies at the cellular and molecular level, which are conducted in this direction, may be able to provide a detailed understanding of the mechanisms of the process and help in optimizing pathogenetic treatment methods. But so far this is only a prospect, not a reality. It should be added that the search for effective ways to help patients with AP over the past many years has not brought tangible success. A certain surge in the improvement of results was observed with the release of new antibacterial drugs, but their use was invariably accompanied by a tendency to decrease the achieved primary effect. At the same time, the former centuries-old experience of medicine remains forgotten and unexplored. A comparative evaluation of the effect of some of the ancient techniques mentioned above using objective tests has shown their amazing ability to bring a positive result. The rationale for new approaches to the treatment of this category of patients has been tested in the clinic and has demonstrated excellent results, fragments of which have been published in numerous articles in recent years and summarized in a monograph [27].
Today, medical science has much more opportunities for an objective assessment and selection of adequate methods of medical care than during the above-mentioned work. It is unlikely that for patients with AP, the old medical care options may be unacceptable if their use allows you to quickly and effectively eliminate the disease. To implement these projects, the results of which are urgently needed by millions of patients, it is necessary first of all to take a critical look at modern views on this problem, bringing the existing ideology of the disease in line with the facts of medical practice and the canons of science. Only after this step it will be possible to choose the optimal therapeutic methods – ancient or recently discovered.
References
Abstract
Two student researchers, one in middle school and the other in grade school, designed and executed an experiment to explore the different factors that other young people use when shopping for food for adults. Using a templated experimental design (BimiLeap), augmented with artificial intelligence, the researchers developed four questions and four answers (elements) to each question. The raw material for the study comprised the 16 elements combined by experimental design into 24 combinations, or 4950 vignettes tested across 100 respondents. The deconstruction of the responses by regression, followed by clustering, revealed two dramatically different mind-sets (focus on the experience of shopping versus focus on nutrition and healthfulness of the food). A third mind-set showed little polarization of responses. The study shows the potential of exploring topics of the everyday by students in grade and middle school, who bring a new perspective to a topic.
Introduction
The world of food selection and food consumption is replete with data, knowledge, insights, and practices. The reason for the abundance of knowledge is obvious; our very existence, and certainly our civilization is predicated on the smooth running of the world of food. And so a detailed review of the literature about food as an introduction to the topic of critical thinking about food ‘behavior’ is not necessary. What might well be a contribution is a study on how young people think about one or another ‘granular’ areas of food behavior. It is in that spirit that this paper focuses on ‘what do people think about the different factors involved when shopping for food?’
The literature on shopping suggests that children are 2-3 times more likely to be mentioned as the source of foods to be purchased in the store. Whether or not the child does the actual shopping, it is the child who exerts a great deal of influence. According to Kraak & Pelletier (1998) “Parents are two to three times more likely to name a child—- not themselves—-as the family expert for selection of fast food, snack food, restaurants, and new breakfast cereals. Market research reveals that children and teenage youth identify products more frequently by brand name rather than food category.”
Much of the information about shopping comes from questionnaires, with the information based upon one’s memory of who did what, and why. Gram (2010) points out that a great deal of what is assumed to be fact may not be as definitive as desired. There is little in the way of experimentation about shopping, and the experiments are often tied to a specific issue, done for a corporation, and stored in the corporate vaults until discarded. In Gram’s elegant questioning of what is presumed to be known “It is well documented that parents know that their children influence what they buy in supermarkets but it is also found that parents and children do not agree on just how much influence children have. Thus, a gap exists in the knowledge about what is actually happening in this grey zone of grocery shopping which seemingly cannot be solved through retrospective data collection. Family shopping is neither a completely rational nor conscious process, which makes the use of self-reported behaviour problematic.”
The origins of this come from separate roots. A literature search reveals that as far back as 2012, Bucknall (2012) published the results of a four-year practical effort to engage children in research. The volume is appropriately titled: Children as Researchers in Primary Schools: Choice, Voice and Participation. Bucknall presents the book as a challenge and a solution.
“How often do your primary school pupils have the opportunity to engage in open-ended, sustained pieces of work that offer them choice and control?
Do you find that the curriculum restricts openings to provide your pupils with real challenge? Is your school grappling with finding effective ways in which to elicit authentic pupil voice? ‘Children as Researchers in Primary Schools is an innovative and unique resource for practitioners supporting children to become ‘real world’ researchers in the primary classroom…. Children in primary schools are accustomed to being set short-term goals and are often unaware of long-term aims or of the connections between the concepts and skills they are learning. In contrast, this book demonstrates that children engaging in the research process have authentic opportunities to apply invaluable personal, learning and thinking skills while managing their own projects, making their ‘voices’ heard and experiencing increased levels of engagement and self-esteem.”
The origin of this paper comes from the ongoing efforts both to empower young people to become researchers by developing their faculty of critical thinking, and by using the opportunity to explore a topic from the point of view of a young person. That topic is what might a person think about when shopping for food. What makes the approach ever relevant is that we rarely explore topics of human thinking and behaving from the point of view of a young person. Even in those situations where we are interested in the response of young people, the process is bounded by the fact that the thinking going into the project is adult-driven. Adults choose the test stimuli. The young person provides data about topics relevant to being a young person, but with the test design by adults. Thus, to address the topic sentence of this paragraph, we are exploring the subject of food shopping, with test materials designed by a student in middle school (CLM, age 14), aided by a student in grade school (CIM, age 8) , and with respondents ages 13-24.
Mind Genomics
The research process is Mind Genomics (Moskowitz, 2012; Moskowitz & Hartmann, 2008). Mind Genomics is an emerging science, dealing with the perception of and decision about topics of the everyday. Mind Genomics emerged in the 1980s, its origin in the business world, where it was becoming increasingly important to create a science of decision-making. This science had to deal with the ordinary, the topics of which were and remain relevant to science. It was the sheer ordinariness, which was relevant, a relevance becoming increasingly important in the business world. The science of the day was and remains the study of decision-making, with, however, the surrounding features of the topic changed so that deep principles can emerge from the experiment. The reality of the situation had to be modified to reveal the underlying process of the way people think, and the way people make decisions. The foregoing paragraph can be summarized simply. That summary phrase is that every day is simply too complex, too unruly, to be of interest to experimental science.
With the inability of experimental science to deal with the complexities of the simple everyday, a different approach was necessary. Fortunately, the approach could be crafted by combining three different disciplines:
Study Specifics
Mind Genomics studies are created using a templated system (www.BimiLeap.com). The system is set up to acquire the necessary information from the researcher, as well as to aid the researcher who needs guidance to provide the necessary inputs (questions, and answers).
Step 1 – Record the ‘Topic’
This portion is simply to give the study a name and to accept the terms of privacy.
Step 2 – Generate Four Questions
The questions will never be shown to the respondents who participate in a Mind Genomics study. The sole reason for the questions is to structure the vignettes so that the vignettes tell a story and to elicit from the researcher different answers to the questions. Figure 1 shows the request by the researcher for the embedded artificial intelligence, supplied by OpenAI (2023) to provide suggested questions. For researchers, the Idea Coach itself ends up being a teacher because the Idea Coach returns with up to 30 questions for each request. The researcher need only write a sentence or two in the specially designated ‘box’, with Idea Coach returning 30 new elements. Figure 1 shows some of the Idea Coach output for an iteration in Step 2. Figure 2 shows the four questions selected by the researcher from the Idea Coach offerings, and after slight editing by the researcher.
Figure 1: Partial output from Idea Coach in response to the request ‘Tell me about young people and buying food’.
Figure 2: The final four questions selected by the researcher
Step 3 – Develop Four Answers for Each Question
Most researchers using BimiLeap find that by the time they have developed the questions, they experience little difficulty answering each question. Nonetheless, Idea Coach provides about 15 candidate answers for each question. When the Idea Coach is instructed to provide new sets of 15 candidate answers for a question, it will return with a number of new answers. Idea Coach thus becomes a teaching aid for the researcher. Figure 3 shows a set of four answers to question #3. The answers emerged from Idea Coach, but the researcher changed the format of the answer by putting the aspect of the question (healthful and nutritious food), followed by a colon, and then the actual answer. The ability to combine the sourcing of the element by Idea Coach with the ability to edit the element to be appropriate for the question becomes an opportunity to reinforce critical thinking.
Figure 3: The four answers provided by Idea Coach, after being edited by the researcher
Step 4: Finalize the Questions and the Answers (Elements)
Table 1 shows the four questions and the four answers for each question. The researcher has edited the questions and answers (now called elements). Note that the answers have been edited for clarity. The original answers emerging from the Idea Coach had relevant information, but the structure of the phrases would not work in a Mind Genomics study, where the elements would be combined ‘as is’, with no polishing at all applied to make the combination easy to read. In light of the recognition that the elements have to ‘stand by themselves’, the researcher polishes the element, so that the first part of the element gives the idea, followed by a colon, and then the specific aspect. This editing did not do any violence to the element but ensured that the element would be meaningful when it would be presented.
Table 1: The questions and elements
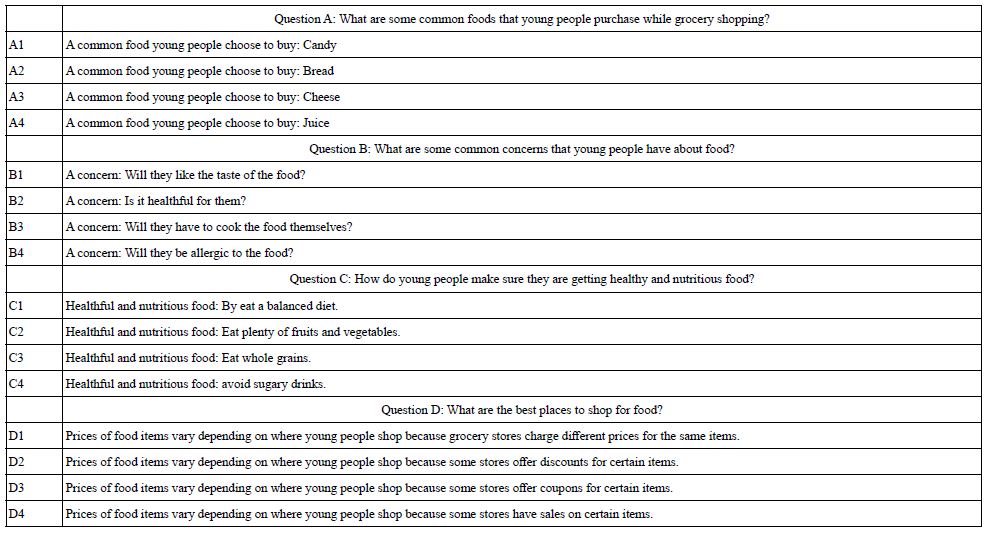
Step 5: Create the Introduction to the Respondent and the Rating Scale
In the actual Internet session with real people, the respondent will evaluate combinations of answers (viz., so-called vignettes). Step 4 instructs the respondents to read (the vignette), and assign a rating on an anchored 5-point scale. The rating question is kept deliberately vague, to let the elements themselves drive the response. In that way, the researcher can determine which elements do the ‘convincing.’
Step 6: Create the Self-profiling Classification Question(s)
The rationale here is that it is often of interest to do the analysis at a granular level. Consumer researchers especially focus on responses to questions, and how different types of people respond to the same question. Through the analysis of the same questions by different groups, consumer researchers often discover new patterns which do not emerge when all the data from all the respondents are combined. The self-profiling questionnaire requires the respondent to define age and gender (fixed for all studies), as well as answer the question below:
Preliminary question: Are young people responsible enough to buy food for older people?
Answers: 1=Yes, they are 2=No, they aren’t.
Step 7: Use the Built-in Experimental Design to Create the Vignette, and Test Them with Respondents
The objective of Mind Genomics is to determine the degree to which the individual elements drive the ratings. At the same time, the respondent evaluates more ‘natural’ combinations of elements, with these combinations constructed according to an underlying set of specifications, known as a permuted experimental design. The design specifies exactly 24 combinations, vignettes, for each respondent, some vignettes comprising two elements, some comprising three elements, and some comprising four elements. The vignettes follow a mathematical structure set up so that the data for each respondent who participates can be analyzed by regression to reveal the contribution of the individual elements.
Step 8: Work through an Online Aggregator of Respondents to Get 100 Respondents
The typical price for easy-to-find respondents may go from a low of US$2 when one provides one’s own respondents, e.g., students, to US$4 when one uses the services of Luc.Id, the aforementioned panel aggregator, to provide respondents It is not advisable to run important studies using one’s own students, simply because executing the study with one’s friends and neighbors can require a week or two when the students provide their own panelists. A more unique approach uses the online panel provider, which may be slightly more expensive but it moves the research as.
Initial Results – Frequency of Ratings
Mind Genomics produces a great deal of data, albeit with each of the test stimuli being unique, perhaps appearing one to three times across the 2400 vignettes generated by the 100 respondents. Our first analysis considers the frequency of assignment of each of the five ratings to the full set of vignettes. We begin by assuming that we know nothing about the meaning of each vignette. We look at the surface patterns emerging, specifically the relative frequency (percent) used by each of the groups that we can identify. These groups will be based on WHO the respondent is, how does the respondent THINK (mind-sets, to be discussed later), and two aspects of the test stimuli, namely the order of testing broken out into four equal positions, and then the speed of response for the assignment of ratings.
When we do this type of analysis, not knowing anything profoundly about the stimulus, we simulate what is often the case indeed what ends up being typical. Table 2 and 3 suggests that without knowing anything more than the information about the respondent, or some superficial information about the test stimulus (viz., position in the set of 24; the speed of response when rating the vignette) we will discover very little from simply deeply analyzing the superficialities of the stimulus [1-9].
Table 2: The rating question and the anchored 5-point rating scale

Table 3: Percent of time respondents select each rating scale point, as well as percent of time respondents choose to say ‘makes no sense’ (BOT2) or ‘makes sense’ (TOP2).
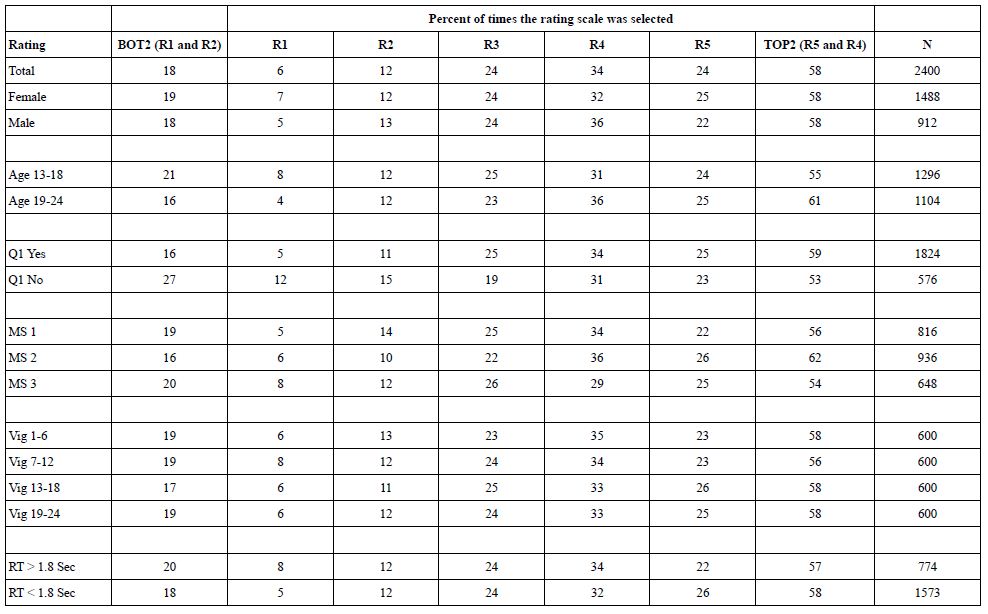
Creating a Database, and then Estimating Equations that Show How Elements ‘Drive’ Ratings
The underlying experimental design provides us with a number of benefits, the most important of which is that the researcher can easily determine the contribution of each element to the ratings. The respondents each evaluated unique sets of 24 vignettes, assigning a rating to the vignette. The data for each vignette was added to a simple database. The creation and properties of that database would be the key to deep understanding.
The database emerges from the following straightforward steps. One need only think of an Excel® worksheet to get an idea of what the database looks like. Here are the different sections of the database. Keep in mind that each respondent will generate 24 rows, one row for each vignette with a separate column assigned for each piece of information.
Section A: Row number. This section comprises a single number from 1 to 2400, to identify the record, and to allow the researcher to sort the file so it returns to the original order.
Section B: Information about the person, including a unique identifier for the respondent and separate columns for gender, age, and responses to the single-added classification question. Each person is different. The same information will be repeated a total of 24 times, once for each of the 24 vignettes that the respondent rated.
Section C: Order of the vignette for the respondent. Each respondent evaluates 24 unique vignettes. This column simply shows the order tested, from the start of the first vignette evaluated by the respondent (Order=1) to the last vignette evaluated by the respondent (Order=24). In the analysis, the order of testing will be augmented by a new variable, ‘Quarters’, with Quarters taking on the value ‘1’ for those vignettes tested in orders 1-6, the value ‘2’ for those vignettes tested in order 7-12, etc. This reduction will enable us to compare the response to the elements when the element was tested in different places, e.g., at the first part of the interview versus at the last part of the interview. Thus, the so-called ‘order effect’ can emerge and be measured.
Section D: 16 columns, one column reserved for each of the 16 elements. For any row (a vignette), the cell corresponding to a specific column is coded ‘0’ when the element is absent from the vignette and coded ‘1’ when the element is present in the vignette. The row will have 2-4 cells with the value ‘1’, and the remaining cells with the value ‘0’. This method is called ‘dummy variable coding’, denoting simply whether a variable is present or absent in a vignette. It will be this coding that allows the statistical analysis of the data.
Section E: The information recorded by the Mind Genomics program, www.BimiLeap.com, during the evaluation of the vignette. The program records both the rating and the response time (RT). RT is defined as the number of seconds to the nearest hundredth of a second elapsing between the presentation of the vignette on the screen and the rating.
Section F: Transformed ratings. Although it is easy to measure responses on a simple scale, such as the 5-point scale used here to assess ‘makes sense’, the reality is that the user of the data often has a difficult time working with the averages or distributions which emerge. The oft-heard question by the manager usually comes out as ‘please explain what this average value of 4.1 actually means, and what actions should I take when I see this average, versus when I see a smaller average such as 2.9?’. Managers who use the data find it easier to deal with yes/no information. To make the data more useful, the Mind Genomics program follows traditional paths previously done in consumer research, viz., recodes or transforms the data. There are two transformations:
TOP2 (Makes sense), ratings 5 and 4 transformed to 100, ratings 1,2,3 transformed to 0
BOT2 (Makes no sense), ratings 1, 2 transformed to 100, ratings 3,4,5 transformed to 0
To prepare the data for statistical analysis it is necessary that the newly created variables (TOP2, BOT2) exhibit some small variability, and not be the same for any individual respondent. To ensure this minimal variable, the BimiLeap program automatically adds a vanishingly small random number (< 10-5) to all newly created values of TOP2 and BOT2, respectively. The number will not measurably affect the results but will protect against ‘crashing’ the statistical analysis program (Regression Modeling).
Once the database is complete, the data are ready for analysis. The ‘workhorse’ procedure is known as dummy variable regression analysis, using OLS (ordinary least-squares) estimation. The analysis estimates the 17 parameters of the equation below:
Transformed Rating=k0 + k1(A1) + k2(A2) … k16(D4)
The early-stage effort to create vignettes according to an experimental design now creates benefits in the analysis. The foregoing equation can be created at the level of each respondent, using either TOP2 or BOT2 as the dependent variable. In turn, the equation can be estimated for any subgroup of respondents, or even any subset of ratings (e.g., for vignettes evaluated rapidly versus vignettes evaluated slowly; vignettes appearing in each of the four ‘quarters, viz., vignettes evaluated in positions 1-6 versus positions 7-12, and so forth).
Parameters of equations for the total panel and for self-defined subgroups appear in Table 4. The table shows the additive constant (k0) and the coefficients for the 16 elements. The table shows only coefficients having a value of +2 or higher. Zero and negative coefficients do not necessarily mean that the elements ‘make no sense’, but rather mean that the element ‘does not clearly make sense.’ Eliminating the negative coefficients allows the patterns to emerge. Finally, strong performing elements, with coefficients of +8 or higher,’ are shown in shaded cells.
Table 4: Parameters of the equation for TOP2 for Total Panel and key self-defined subgroups
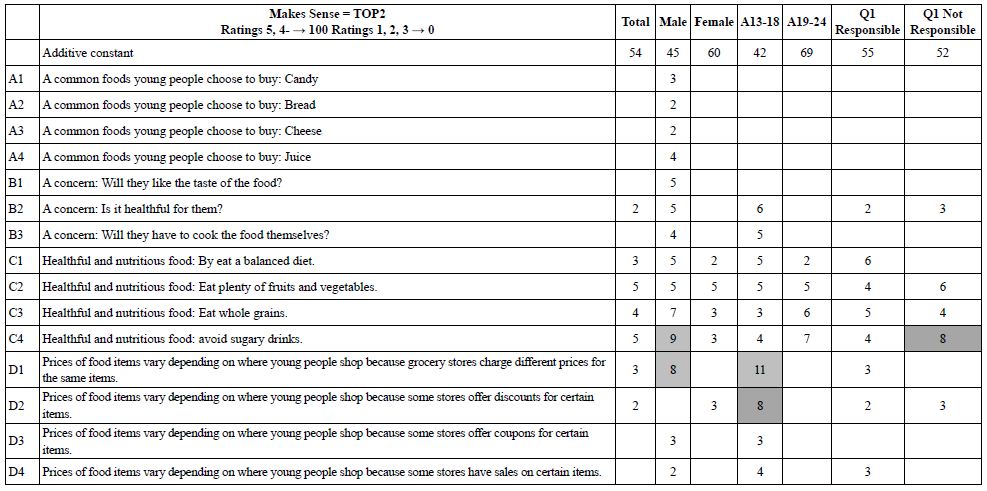
Our first pass through the data focuses on the additive constant. The additive constant shows the likelihood to say that the vignette ‘makes sense’ in the absence of elements. Of course, the underlying experimental ensured that every vignette comprised 2-4 elements so that the additive constant is a computed parameter, one that we can use as a baseline. The data shows interesting patterns. The total panel shows an additive constant of 54, meaning that in the absence of elements we might expect 54% of the ratings to be 5 or 4, viz. TOP2. When we look at the genders, however, we see that males are less likely to say ‘makes sense’ (additive constant 45), whereas females are more likely to say ‘makes sense’ (additive constant 60). We see the same pattern emerging by age. The younger respondents show a much lower additive constant than the older respondent (additive constant 42 for ages 13-18 vs. 69 for ages 19-24). Finally, when the respondents are asked whether young people are sufficiently responsible to buy food for older people (Question #1), the additive constants are very close (55 versus 52).
It is in the elements that we see differences among the group. The first thing to keep in mind is that the elements are departures from the baseline. Thus, with a low baseline, there may be few positive elements or any positive elements. The reason is that with a low baseline, there may be a few strong-performing vignettes, but most perform poorly. With a high baseline, there are generally few strong-performing elements, moving beyond the already-high level. There may be many negative elements, but these will not appear because we are only looking at positive coefficients.
With the foregoing guidance, we see that males and respondents ages 13-18 show the largest number of positive coefficients, a pattern that is to be expected given their low additive constants.
There are a group of strong-performing elements
C1 Healthful and nutritious food: By eat a balanced diet.
C2 Healthful and nutritious food: Eat plenty of fruits and vegetables.
C3 Healthful and nutritious food: Eat whole grains.
C4 Healthful and nutritious food: avoid sugary drinks.
D1 Prices of food items vary depending on where young people shop because grocery stores charge different prices for the same items.
D2 Prices of food items vary depending on where young people shop because some stores offer discounts for certain items.
Our second pass through the results looks at the pattern of coefficients for elements appearing in vignettes at the start of the session (vignettes 1-6) versus elements appearing at the end of the session (vignettes 19-24), as well as elements appearing in vignettes evaluated quickly versus vignettes evaluated slowed (operationally different as response times >1.8 vs. response times >1.8 seconds). Table 5 shows the parameters. There are differences by groups. The only strong, consistent pattern to emerge is that the elements presenting ‘health and nutritious food’ makes much for sense at the end of the evaluation than at the beginning of the evaluation. It may be that these messages must be repeated, at which point they begin to make more sense.
C1 Healthful and nutritious food: By eat a balanced diet.
C2 Healthful and nutritious food: Eat plenty of fruits and vegetables.
C3 Healthful and nutritious food: Eat whole grains.
C4 Healthful and nutritious food: Avoid sugary drinks.
Table 5: Parameters of the equation for TOP2 for the first six versus the last six of the vignettes tested, as well as the vignettes rated quickly versus the vignettes rated slowly.
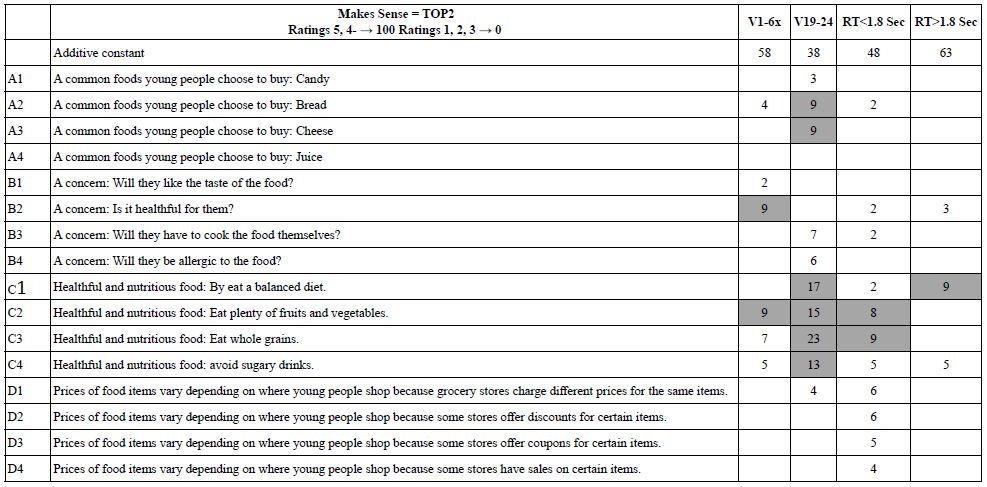
The second set of columns shows the results for the vignettes rated quickly (RT<1.8 seconds) and the vignettes rated more slowly (RT>1.8 seconds). The additive constant for the more quickly rated vignettes is lower (48 for RT<1.8 vs. 63 for RT>1.8). This difference suggests that people may reject more quickly, versus accept more slowly. The rationale for this conjecture is that the lower additive constant for the vignettes rated quickly.
Of importance is that the strong performing elements are three of the four examples of nutritious foods.
C1 Healthful and nutritious food: By eat a balanced diet.
C2 Healthful and nutritious food: Eat plenty of fruits and vegetables.
C3 Healthful and nutritious food: Eat whole grains.
Our final pass through the TOP2 data for ‘makes sense’ involves the discovery of underlying groups of people who think differently about the same topic. These groups are called mind-sets. These mind-sets emerge when the researcher looks at the pattern of coefficients for a single topic, like the topic we investigate here, viz., making sense about buying food. The mind-sets emerge clearly when we use statistical methods to find these groups. The method is called ‘clustering.’ For the study, we use so-called k-means clustering to separate out the 100 respondents first into two groups, and then into three groups, based solely on the similarity of patterns of the 16 coefficients.
The clustering program looks for different groups by creating a measure of ‘distance’ between each pair of respondents. With 100 respondents we have 100×99/2 or 4950 pairs. The distance between two test respondents in this study is defined as the quantity (1-Pearson Correlation). The distance is 0 when the two respondents show exactly parallel patterns of coefficients. The distance e is 2 when the two respondents show exactly inverse patterns. The clustering program does not care about whether or not the clusters make sense. That is the researcher’s job. The clustering program is simply a mathematical tool (Likas, 2003).
The researcher’s job is to select the most meaningful cluster solution from the solutions generated by the clustering program. The two criteria are parsimony (few clusters are better than many clusters), and interpretability (the clusters must make sense, viz., tell a coherent story)
Table 6 suggests two strong clusters (Mind-Set 2 and Mind-set 3), and one weak cluster (Mind-Set 1). Mind-Set 2 focuses on the actual shopping behavior. Mind-Set 3 focuses on health. Mind-Set 1 might be folded into Mind-Set 3, but the responses of Mind-Set 1 are weak, suggesting an almost indifferent attitude.
Table 6: Parameters of the equation for TOP2 for the three mind-sets extracted by k-means clustering
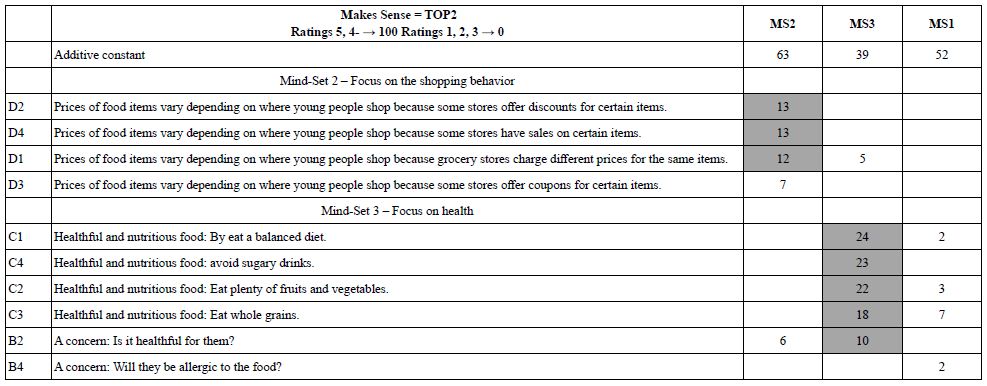
The additive constants for the mind-sets are quite different. Mind-Set 2 focusing on the shopping behavior shows the highest additive constant, 63, meaning that almost 2/3 of the time they are likely to say that the vignette makes sense. They do not seem to be particularly critical in the way they think. In contrast, Mind-Set 3 focusing on the healthfulness of the food shopped for shows the lowest additive constant, 39, meaning that only 40% of the time are these respondents likely to say that something makes sense.
Discussion and Conclusions
The study reported here demonstrates the ease with which students can investigate topics of everyday in a way that combines the joy of research and learning with the unbounded curiosity and enthusiasm of young people. One might consider the actual topic itself to be simple, not grounded in theory, and certainly not conducted with the gravitas of a ‘serious scientific experiment’, which often responds to so-called ‘question emerging from the literature’, or even more colloquially, research which fills a hole in the literature.
The topic of food choice is a serious topic, one relevant to well-being and to illness alike. Malnutrition is a worldwide problem, whether the poor nutrition comes from a lack of food, a lack of knowledge, or just bad eating habits. Many of the studies appearing in a rigorously scientific way address the topic, but in what ends up being an episodic, punctate fashion, each paper exquisitely analyzed in its own way, with a depth of information designed to demonstrate its inherent ‘scientificity’ (sic). The deeper information, the emergence of patterns leading to application, ends up being the job of the individuals doing ‘meta-research’, writing review papers, summarizing what is known, and then prescribing where appropriate.
These studies with Mind Genomics, augmented by artificial intelligence (REF) designed and executed by young researchers move science in a different, parallel direction, perhaps one reminiscent of the early days of science. It is the excitement of the unknown, the exploration of topics, the discovery of aspects of how people think, and the curiosity of youth that drive this new approach to science. And, there is the other side, the discipline in development, execution, and analysis of the data afforded by the Mind Genomics process, the remarkable simplicity, speed, and low cost of the approach, which when combined allow anyone in the world, or at least anyone with sufficient curiosity, to create a large-scale database of different aspects of a topic, such as food shopping. One can only imagine 100-200 studies of this type, with different sub-topics of food shopping, with different age people, in different regions of the world, at different times of the year. Such a dataset is simple to erect, and fun to do so, especially when the researchers are students from different schools, countries, and cultures, all cooperating on a platform design to make these types of Mind Genomics studies easy to do.
Acknowledgments
We gratefully acknowledge the sponsorship of our colleagues who support these studies to help students develop critical thinking, and thank our fellow students for the chance to discuss the topics with them.
References
Summary
In Cameroon, the number of people with disabilities is estimated at nearly two million nine hundred and ten thousand (2,910,000). Thus, a little over 5% of the population of Cameroon suffers from at least one disability [1]. These alarming figures lead us to consider the issue of children’s disability and its impact on the health of their parent(s). Certain types of disability cause more suffering to caregivers and relatives than to the disabled person. Within the framework of our activities in clinical psychology with associations of parents of children living with disabilities, through clinical interviews with parents of children with Down syndrome and autism, we have observed that many of these parents present various forms of psychopathology related to the disability of their children: affective disorders, depressive anxiety disorders, acute stress, behavioral disorders, PTSD, etc. We wondered how to deal with these suffering parents. To answer this question, we administered the SPRINT (a recent traumatic event assessment scale) to parents of children with disabilities whose discourse highlighted their experience with their different child as traumatic. This evaluation allowed us to set up therapeutic projects with EMDR (Eye Movement Desensitization Reprocessing). Through a reading of seven clinical cases followed in Yaoundé, Cameroon, we were able to verify that EMDR psychotherapy is a useful care tool for the management of parents of different children in pain. For most of the cases, the first EMDR session was very satisfactory. The results obtained were astonishing: 04 parents saw their VOC (truth scale) rise to 7 and their SUD (suffering scale) drop to 2 at the end of the first EMDR session. For the 03 other parents, the VOC rose progressively over the course of the sessions to reach 7 at the sixth session with an economic SUD at 1, due to their sometimes traumatic childhood experiences.
Keywords
Disability, Child with a disability, Psychopathology, EMDR, PTSD, SUD, VOC
Disability and Society
Society is a group of men and women who are united by nature or by laws. These laws differ from one sphere to another. Thus, what is seen as taboo in one society may be normal in another. However, there are common features between societies with regard to the concept of norm. This norm is applied to each individual who, for the most part, is subjected to it without any choice. Those who deviate from this pre-established norm are considered a problem, a social case. It is in this logic that the person living with a disability fits in. “Disability” is used here as an umbrella term for impairments, activity limitations and participation restrictions that represent the negative aspects of the interaction between a person (with a condition) and contextual factors (personal and environmental). Disability is neither a purely biological nor a purely social phenomenon” [2]. A person with a disability is therefore a person with physical, mental, or sensory incompetencies that affect their activities of daily living and limit their actions in society. The concept of disability can be defined in several ways depending on the culture and society. In so-called Western societies, disability is seen as incapacity, a lack. However, it should be noted that the concept of disability has evolved in these societies with the scientific progress of the 19th century because it was not always so. In African society, disability is still considered by most people as a curse to be got rid of. In most regions of Cameroon, disability is seen and understood as something mystical, supernatural. With the mixing of populations, a slight evolution of mentalities, the advent of ICTs, and access to education, this conception is changing. 5.4% of the population in Cameroon suffer from at least one type of disability. Sensory impairments (3.6%) are the most frequent, due to (2.2%) for visual impairments and (1.6%) for hearing impairments, followed by motor impairments (1.2%) which are mainly deformities of the lower or upper limbs [3]. According to the same survey, “the proportion of people with disabilities is higher in rural areas (6%) than in urban areas (4%) and “this proportion increases steadily with age, from just over 1% among children aged 0-4 years to 6% among people aged 25-49 years and reaches 19% among those aged 50 years or more.”
Disability and Its Manifestations
Disability is an impairment that limits the subject in the efficient performance of his or her actions. According to the WHO, “disability is universal”. According to the INS and ICF International survey, it is defined as “a disadvantage resulting from an impairment or disability, which limits or prevents the individual concerned from performing a role that is normal for him or her, taking into account age, gender, and social and cultural factors”. The number of people with disabilities is estimated to be over one billion people, including about 15% of the world’s population in general, and in turn, one in seven people [4].
Disability generates clinical manifestations that are often poorly understood. Whether sensory, motor, mental or social, disability always poses a societal problem. The lack of expression of positive emotions by parents towards their children with disabilities is a striking modality of the functioning of families with a child with a disability in Cameroon. Today, many families or parents want to give the maximum to their disabled child. Unfortunately, they face several difficulties or sufferings that can put them at a disadvantage; among others; the gaze of the other, the mourning of the idealized child, the fear of reliving the same experience and the inadequacy of our environment in terms of infrastructure. Whether it is sensory, motor, mental or social, disability almost always poses a problem of social integration. The emotional suffering of families with regard to their children with disabilities is a striking feature of the functioning of families with a child with a disability in Cameroon. In our different actions carried out with the parents of disabled people, we noticed that several parents had psychological illnesses linked to their child’s disability. We wondered if the non-acceptance of a child’s disability could lead to a psychological illness? What can be done to help them? What types of psychotherapies would best respond to their suffering? From these questions arise a series of hypotheses among which the following one. Following a high SPRINT score in these parents, we can use EMDR therapy to treat them and especially to control the impact of the suffering during therapy.
The term disability has several definitions depending on the model (medical and social). Medically, it is defined as an incapacity, a deficiency, a lack, whereas socially, it is defined as an inadequacy. It is for this reason that the WHO, taking into account these two models, defines a disabled person as “any person whose physical or mental integrity is temporarily or permanently impaired, either congenitally or as a result of age or accident, so that his or her autonomy, ability to attend school or to hold a job are compromised. The French law of February 11, 2005 [5] on equal rights and opportunities, participation and citizenship of people with disabilities provides a simpler definition of disability. According to this law, disability is “any limitation of activity or restriction of participation in society suffered in his or her environment by a person due to a substantial, lasting or permanent impairment of one or more physical, sensory, mental, cognitive or psychic functions, a multiple disability or a disabling health disorder. Disability is a social notion rather than a medical one because the person living with a disability needs to move in a society to consider himself as an important being. In short, the term disability refers to the difficulty that an individual encounters in interacting with his or her environment and that is caused by an impairment that results in a permanent or non-permanent inability to access, express, understand or apprehend.
In Cameroon, the population of people living with a disability is estimated at nearly 10% of the 18 million inhabitants [6], a percentage that has doubled in four years since the INS and ICF International survey. To understand the psychological situation of this part of the population, we must invoke the psychology of disability, which condenses the entirety of the psychological needs and experiences of the person with a disability as well as those around them, without ignoring the characteristics related to their life phases. It allows for a better understanding of the needs, adaptation problems and significant interference according to the types of disability situations (motor, sensory, psychological or mental). To make this field of investigation more concrete, let’s look at the role of a psychologist.
The Psychologist in Question
The psychologist is a health professional whose role is to offer the individual a place to listen, to speak, and to maintain confidentiality in order to identify conflicts. He is trained in the psychological analysis of the individual, but also in the analysis of factors internal or external to the individual that influence this psychological functioning. He is an expert in conscious and unconscious psychological functioning. His analysis allows him to understand what is going on in the individual at the cognitive, affective and behavioral levels, contextual and social. To perfect this, he has the appropriate methods, tools and techniques. His essential skills are: psychological evaluation (audits, diagnoses, counseling, training, orientation), clinical interviewing, psychological support, therapeutic management. In this panoply of skills, there is one that allows the specialist to work directly with the patient or individual with a mental health problem.
The clinical psychologist is the one who works at the bedside of the individual. He promotes mental health through prevention, care and reintegration or professional orientation. He/she assesses the people who make a request in order to determine the nature, causes and potential effects of the distress (emotional, physical, social) felt by the person or group. He intervenes in order to prevent, treat and address psychopathologies, emotional conflicts, and skill deficits at the root of the dysfunction. He therefore intervenes for the promotion of health. It is in this movement that the clinician is training in psychotherapy. One of these revolutionary therapies is called EMDR
What is EMDR?
EMDR psychotherapy is a fairly new therapeutic intervention that aims to provide relief to patients with post-traumatic stress disorder by helping them to let go of traumatic memories. EMDR (Eye Movement Desensitization and Reprocessing) is a therapy developed in the late 1980s by Francine Shapiro [7]. With the aim of reducing the emotional charge linked to traumatic events, EMDR thus becomes a powerful tool for “cognitive restructuring”. It is a therapy that is currently used to effectively treat a wide variety of psychological disorders resulting from traumatic memories, including anxiety disorders, depression, stress and trauma [8]. But especially in Post-Traumatic Stress Disorder (PTSD). Shapiro’s theory stipulates that the information linked to the trauma is stored in a fragmented manner (images, sounds, smells, places, events, etc.) in the brain and that these different fragments are not linked together, which prevents the integration of the trauma into the memory. It presents a specific information processing system, which deals with traumatic memories, called Adaptive Information Processing (AIT), so that during the course of our existence, certain information is not processed, and therefore not memorized, which means that it is constantly present in our memory. This dysfunctional information remains unresolved and constitutes dysfunctional memory networks; their voluntary or involuntary recall is unpleasant and painful, and the emotion can arise unexpectedly as soon as the environment recalls the circumstances of the traumatic event. They are the source of various disorders such as intrusive thoughts and images, nightmares, fears, untimely startles, phobias… The objective of the therapy is to promote the transfer of information between the emotional and cognitive brains in order to stop the disorders.
The EMDR Procedure
EMDR combines several methods already used by other approaches. In particular: CBT (cognitive and behavioral therapies), psychodynamic therapies and Ericksonian hypnosis. It consists of eight essential phases: the patient’s life history and treatment planning (collection of anamnestic data, the most distant or most recent memories), the preparation of the patient (targeting plan in agreement with the patient), the evaluation (preparation phase for cognitive associations for the TAI), thedesensitization (bilateral stimulation), settling (positive cognition reinforcement), body scanning, closing and re-evaluation.
When life episodes generate too much emotional disturbance, whether they are small traumas (being humiliated as a child, witnessing violent arguments from one’s parents, etc.), or large traumas (rape, accident, attack, earthquake…), the information processing system is blocked. This leads to the following consequences: post-traumatic stress disorder, depressive, anxiety or eating disorders, drug addiction, various physical disorders… EMDR is based on a neurological model in which the alternating stimulation of the cerebral hemispheres re-establishes a process of re-connecting the elements of information processing (emotional, cognitive, physical) disconnected by the traumatic event. In other words, the adaptive process of information processing could be reactivated by the bilateral stimulations. Once reactivated, this system would process the traumatic material in an accelerated manner. Thanks to this system, negative emotions are neutralized and adaptive information arises spontaneously. EMDR makes it possible to establish a connection between the memory network that contains the traumatic memory and the memory networks that carry the adaptive, incorporated experiences that have meaning for the individual and constitute psychological resources.
The Principle of EMDR Therapy
After having had an initial clinical interview with the patient, the therapist verifies the patient’s problematic using a scale of his or her choice, after which he or she must respect the above-mentioned steps. The patient identifies a representative image of the most disturbing dysfunctional target memory, gives the negative cognition of himself, finds a positive cognition of the same register with a verification scale, identifies the emotions linked to the target, the related body sensations, and above all situates the suffering, the disturbance linked to the event on a scale. The cognitive evaluation of the target dysfunctional memory is done on a subjective scale and the degree of distress in relation to the target memory is evaluated throughout the desensitization phase. During this desensitization phase, the patient returns to the image from the beginning by making a kind of cognitive association, while simultaneously making eye movements from left to right in order to follow the therapist’s hand movements, which act as a dual-action stimulus (either in front of the eyes, on the knees, on the shoulders or beside the ears). After each series of SBA (bilateral stimulation) the patient is asked to report the associative information that was elicited during the EMDR session, the instruction given to the patient is either to move the eyes from left to right, to listen to the sounds produced by the hand, to listen to the vibrations produced by the tapping… at a regular rhythm, while thinking of elements of a traumatic memory.
The EMDR Session
Each classic EMDR session lasts between 45 and 90 minutes. The EMDR treatment begins with a preparation. It is important for the therapist to diagnose the type of trauma (simple, psychic poisoning or complex). The therapist also helps the patient to develop resources, not only to improve his or her relationship with himself or herself and others, but also to facilitate the treatment of the trauma. EMDR allows the brain to reprocess the emotional information in order to remove the trauma from the nervous system. Before beginning the EMDR treatment, the therapist follows the above-mentioned steps. In this way, he/she offers the patient a safe therapeutic space that will allow him/her toto confront the origin of his suffering and especially to take refuge in a comfort zone in case of abreaction.
As Martine Gercault [9] puts it so well Once the foundations of the work have been established, the practitioner will help the patient to locate and represent as accurately as possible the origin of the target event, to feel in his or her body the perceptions, emotions and sensations that are linked to it. While the thoughts and affects surface, the psychotherapist sweeps his or her hand in front of the patient’s face and the patient follows rhythmically with his or her eyes”. The reprocessing of a trauma can take from one to several sessions. To reprocess a traumatic episode, the psychotherapist invites the patient to focus on his or her memory, by being in contact with its sensory elements (visual, auditory, olfactory, kinesthetic, gustatory…), with the beliefs and negative emotions generated. The therapist then initiates a series of alternating bilateral left and right stimulations (30 seconds to a few minutes) of eye movements, sounds or tactile stimulations. As free associations of ideas emerge, the patients reprocess the different information linked to the memory, integrating them into their memory network in a functional, adapted manner. Between each series, the therapist asks the patient to take a deep breath and to share what came to mind during the stimuli. These successive and quite brief series of bilateral movements continue until the emotions are neutralized and the emotional scars of the past are emptied of their traumatic charge. When the traumatic memory is thought of again without emotional discomfort and associated with positive thoughts, the therapist moves on to the next phase. The traumatic memories lose their negative emotional charge, thus ending the suffering and negative reactions. It may happen that during a session, the patient experiences strong emotions; it may also happen that between sessions such emotions resurface, as well as other memories, as in any form of psychotherapy. In the end, the patient experiences an improvement in the emotional disturbance related to the memory being treated, and a calming. Through this process, images, perceptions and memories that were negatively encoded in the emotional brain are reprocessed and lose their dramatic intensity. The past adversity is replaced by the uniqueness of the event.
Procedure for the Parent Survey
The first step taken was to contact the heads of the associations we had identified for our investigation (WellbeingAfrica, an association of parents of children with disabilities that works for the rights of vulnerable people), the Little Prince and the Moabi [P²M], an association of parents of children living with disabilities whose main mission is the empowerment of people with Down’s syndrome and other disabilities). Having obtained the various appointments, we organized ourselves for the meeting with the targeted parents. Once on site, after a detailed explanation of the object of our research, we were allowed to “arrange” an appointment with the parents concerned. On the day of the meeting, we first proceeded with a sort of interactive discussion with all the parents present. The purpose was to give them all the explanations related to the research and to the importance of their participation, especially for their well-being.
After this collective meeting phase, which lasted about 20 minutes, each parent was taken individually in a more private setting of the institution (consultation room or office set up on site). There, we would conduct a clinical interview with the parent to ensure that he or she met the inclusion criteria for our sample. As a reminder, these criteria were: being a parent (father or mother) since birth, having denial of their child’s disability, having a psychological disorder related to their child’s disability, and especially having a high SPRINT score, willingly agreeing to take an active part in therapy… Once these conditions were met, we asked the parent to ask any questions he or she might have about our study. After these preliminary steps we would then make a well-framed appointment for the preparation of the actual therapy.
Post-Traumatic Stress Disorder (PTSD) Clinic
Post-traumatic stress disorder (PTSD) affects people who have experienced trauma caused by violence, disability, accident, natural disaster or war, or degrading treatment. How society views the trauma. Lack of support or negative behaviours of those around them (criticism, blame, lack of understanding and empathy, or hostile, controlling, intrusive or stressful behaviours) aggravate the symptoms. Victims feel painfully judged by others. Support from others is very important. Trauma-related thoughts made by the victim herself.
A set of symptoms can develop in a person following a confrontation with an intense stressful event (loss of an object) that would involve serious injuries or a feeling of helplessness. Such situations sometimes trigger strong anxieties, chills, sweating, trembling; and psychic sides such as dreams, flashbacks and sometimes avoidance of similar situations. The positive symptoms are: reliving, avoidance, negative alterations, neurovegetative disorders. These symptoms cause significant suffering in the person, leading to an alteration in their social and professional functioning, and many other important areas. Thus, the patient’s entire functioning may be turned towards the trauma and its memory. Victims will tend to avoid thoughts and conversations that remind them of the traumatic event, as well as places, situations and people that may remind them of the original situation. Their interests and relationships gradually diminish.
Presentation of the Cases
Case PS
PS is a young married woman of 35 years old, of Catholic religion, of Bamileke ethnicity. Her schooling level is that of the 4th grade. She carries out an informal activity that is very common among women in Cameroon, known as “bayamselam,” which consists of buying food products in bulk at the end of the fields to transport them to the city markets and sell them in retail. She is the third of five siblings and her 15-year-old disabled child is schizophrenic. During the interview, she appeared very distressed. She was born in 2003 in Yaoundé, the first of five children of PS, including one girl and four boys.
Case M
M is a young Cameroonian woman, 42 years old, of Bulu ethnicity, with a BTS level of education and unemployed. She is the first of two girls. She is the mother of J who was born on May 31, 1997. He is the only child of M and suffers from an autistic spectrum disorder.
Case E
E was born 55 years ago to a Christian protestant family in the Sanaga Maritime. She has a CEPE. She is a housewife, married and mother of five children, herself the fifth of seven children. She is the mother of Y, born in 2007 in Yaoundé, the fourth of her five children. 02 girls and 03 boys, she attends a local special school, she has a mental retardation.
Case T
T is a 48 year old housewife. Of the Foulbé ethnic group, she is Muslim, without school education, she is married and mother of seven children. She is the sixth of nine children. She is the mother of J, born in 2007, who is the first of these 07 children, of which 03 are girls and 04 are boys. He has been in the special SIL for three consecutive years.
Case X
X was born 45 years ago and is of Douala ethnicity. Catholic, with a literary baccalaureate, he is a service provider. He is the first of three siblings, including two boys and a girl. X is the father of K who was born in 1998. He would suffer from an autism spectrum disorder.
Case P
P is a 30 year old Gabonese, of Fang ethnicity, catholic, he holds a BEPC, he is a military man by profession and single with two children, he is the second of three siblings. He is the father of B who was born in 2002 in Yaoundé, the first of 02 boys and he is being trained in a specialized school in the area. He has been suffering from schizophrenia for two years.
Case Z
Z is a 38 year old housewife, of Bulu ethnicity, from the evangelical church, with no school education. An only child, she is married and has three children. The disabled child is the third of 8 years old, autistic, and attends an inclusive school in the area.
Analysis of the Data Collected during EMDR Therapy
Seven parents were recruited on the basis of individualized clinical interviews among the parents of children with disabilities, including five (05) mothers and two (02) fathers from associations of parents of children with disabilities in Yaounde. Before starting the therapy, we made sure of the type of trauma that each parent might have, because the arrival of the disabled child could be just the trigger for the suffering. After each session, we administered a Stressful Event Rating Scale (SPRINT) to the parent to assess the effectiveness of EMDR therapy. By doing this, we were able to treat all seven parents according to their individual schedules, over a period of 2 months, with an average of 5 sessions of 60-90 minutes each (Table 1).
Table 1: Analysis of the data collected during EMDR therapy
|
Most Disturbing Image |
Negative Cognition |
Emotion |
Body Sensations SSC |
SUD |
Positive Cognition |
VOC |
|
| PS | Haunting voice | I am a bad mom | Crying, sadness | Pain in throat and heart palpitations | 9 | I am a good mom | 3 |
| M | Vision of agressive child | I am the worst of all | Crying | Headaches | 10 | I am among the best | 2 |
| E | Sight of a normal child | I am sick | Sadness | Jerky breathing | 8 | I am a human with limits | 2 |
| T | The sight of an inhuman | I am a monster | Crying | child Pain in the lower limbs | 9 | I am human | 1 |
| X | A difficult delivery | I am an incompetent father | Sadness | Tachycardia | 7 | I am a good father | 3 |
| P | Nightmares | I suck | Crying | Sweating | 9 | I am capable | 1 |
| Z | A beautiful but hyperactive baby | I am a bad mother | Sadness | Sore throat | 8 | I am a good person | 2 |
An insecure family context, a feeling of guilt related to a probable negligence during the pregnancy and the development of the disabled child, stereotypes, accusations and stigmatizations coming from the entourage, lack of projection in the future, feeling of devaluation, the look of others, the physical manifestations are the elements that emerge from the discourse of the different parents.
Clinical Case PS
For EMDR therapy, we need 08 phases: the life history of the subject, the assessment, the desensitization, the reinforcement of positive cognition, the body scan, the future scenario, the closure and the reassessment.
Clinical Aspects of the Test
The relationship with the clinician being well established, PS presents her apprehensions, suspects at the beginning of the manipulation as she declares “I trust you docta, even as I don’t know what I’m getting into, this doesn’t seem catholic to me, looking from left to right there scares me”. In spite of this, she lends herself to the game and respects all the instructions given for the good progress of the EMDR therapy.
The encounter with the therapy device immediately provokes a movement of surprise in PS. She smiles when I explain the course of the session. Regarding the eye movements, she said to me: “Docta, excuse me, but I am going to laugh”. This observation is recurrent with EMDR patients, because it is different from what they expect, not only do we not only do active listening or give them advice, but we also ask them to make eye movements, and to verbalize what comes to their mind during desensitization.
The Subject’s Life Story
PS is a young woman of 35 years old, of Catholic religion, of Bamiléké ethnicity. Her school level is that of the 4th grade. She is the third of five siblings and her 15-year-old disabled child has schizophrenia. Her score on the SPRINT test by Connor & Davidson 1997, translated by F. Mousnier – Lompré 2014 is 18. We made a targeting plan and listed 02 targets: The first is a conflict with her father because she never felt loved by him. The second is her child’s disability. With her permission, we started the therapy with the current situation, which is her child’s disabling illness.
Assessment of the Situation
The elements of the therapy are: the image which is the haunting voice of her daughter in crisis, the negative cognition “I am a bad mother”, the positive cognition “I am a good mother”, the VOC equals 2, the emotions are crying and sadness, the SUD equals 9 and as body sensation the pain in the throat and the heart palpitations.
Desensitization
This phase is marked by bilateral stimulations, breathing movements and especially by adaptive information processing (AIT). PS’s speech reveals an increased suffering following her daughter’s diagnosis. She revisits her childhood, her friends, her family, her marriage, in short, all the important elements of her life and notes a major fact that justifies her discomfort. Her behavior when she was young, she says in these terms: “I see myself with my brother making fun of people with a physical handicap, especially the neighbor’s son who had a limp”, “I can’t live with a handicap or put up with a person with a handicap”. As the therapy progressed, she understood that she did not have the right to decide for anyone, that life had its elements that she had to accept and deal with, that she had regained her values and, above all, that she had found meaning in all the efforts she had made since her daughter’s diagnosis, in all the appeals she had had to make for the child’s well-being, and, above all, that she had been a good mother because she had not abandoned her child in her situation of psychological illness. When the SUD drops to 1 economic, we move on to phase 5.
Reinforcement of Positive Cognition
We just check the positive cognition that she gave at the beginning namely “I am a good mother”, when the VOC goes up to 7, we go to phase 6.
The Body Scan
In a relaxing atmosphere, we go over all the parts of her body, always coming back to the disturbing image that we no longer name in this phase. We just say to him, thinking back to the starting image, and especially to the negative cognition that you stated at the beginning, we are going to do an examination of your whole body starting from the head, the neck… to the toes. The instruction is simple: every time she recently feels a knot, a pinch, a pain, an affect in any part of her body, she reports it to us and we desensitize. She has reported pain in her throat and neck and each time we ask her after the desensitization: “what came to mind”, until we get zero pain or manifestations in the body. Once the VOC is verified, we change phase.
The Closing
After having informed Mrs. PS that we will soon stop the session, we say to her: “you have worked well today, I encourage you to note down everything that appears in the meantime, you can report them to me at our next session”.
Reassessment
This session allows us to make a small evaluation of the previous one in order to desensitize the new elements if there are any. After six sessions, we have allowed Mrs. PS to have another look (admiring) on her child.
Results
The action of EMDR is based on the association of psychological and neurological processes. This technique allows the patient to revisit a traumatic event. This therapeutic action is understood as an information processing therapy during which the patient recounts the traumatic event by means of its cognitive, affective and physiological characteristics while concentrating visually, audibly on bilateral movements of an external stimulus until the psychological distress evoked by the traumatic memories diminishes or disappears (Shapiro, 2001).
We have experienced this in the seven parents who, after just two months of care, regained the smile they thought was lost forever. For most of the cases, the first EMDR session was very satisfactory for the parents because 4 of them saw their VOC rise to 7 and their SUD drop to 2. For the other 03 parents, the VOC rose progressively during the sessions to reach 7 at the sixth session with an economic SUD because of the sometimes traumatic experience of these parents.
Discussion
Contrary to other types of therapy which are all equally effective, EMDR has the particularity of not expecting patients to verbalize and perform precise tasks which will constitute the action of the treatment received. The effects of EMDR are less prolonged than cognitive and behavioral therapies, which facilitates the rapid recovery of parents who cannot feel good just by verbalizing their suffering. The main advantage of EMDR lies in the brevity of the application of this technique. Indeed, when properly indicated, it acts directly and shows positive effects in the first session. EMDR has been used in randomized controlled studies with a waiting list where placebo control groups show a definite therapeutic effect [10].
Conclusion
Our work highlights the action of EMDR therapy on the psychological problems of parents of disabled children. For these parents at the end of the therapies, each parent, who at the beginning felt a fair amount of suffering at the sight of his or her disabled child, found himself or herself satisfied with his or her life and, above all, found qualities to be amplified in order to consolidate each of his or her different child’s achievements. The results are very satisfactory.
The treatment is essentially psychosomatic and global. It would be interesting to verify the stability of the results in a few years by observing the parents concerned over the years. In the field of brief and effective therapies, EMDR is one more tool that seems promising.
We did this study in 2019, to check the sustainability of the therapy, we did an evaluation three months for each one after stopping the therapy and one year after. The advantage was that we stayed in contact with the parents in question.
References