DOI: 10.31038/IJVB.2021524
Abstract
Lymphoma is the hematopoietic tumor of higher incidence in domestic cats. Myelosuppression is the most remarkable side effect of the conventional treatments for this disease, especially for patients with debilitating infections such as FIV and FeLV. In this context, alternative therapies could be recommended for treating lymphoma as a sole therapy or even in association with conventional therapies to provide a better quality of life to the patients and fewer side effects.
Material and Methods: A 4-year-old neutered male mixed breed cat was seen at NaturalPet Clinic in Brazil. The cat was positive for FIV and FeLV, diagnosed with lymphoma, and had relative difficulty breathing and swallowing. On the physical examination, a nodule was observed in the right ventral part of the tongue. An incisional biopsy was performed for histopathological analysis, and the lymphoma diagnosis was confirmed. The disease was treated with homeopathic medicines, such as daily applications of Viscum album in the D3, D6, D9, D12, and D30 dilutions. Complete remission of clinical signs was observed after completing the treatment period with the reestablishment of the patient’s health.
Conclusion: The homeopathic treatment used in this case allowed the disease resolution, had no side effects on the patient and increased his life expectancy.
Keywords
Cancer, FeLV, FIV, Viscum album
Introduction
Lymphoma can be defined as neoplasia of lymphoid tissues or lymphosarcoma. It primarily attacks lymph nodes and/or other solid organs, such as the spleen, liver, or thymus. It can also affect no lymphoid tissues [1]. Neoplasms of hematopoietic origin can be considered the most frequent among domestic cats [2,3], and the most frequently diagnosed neoplasms representing about 90% of tumors in this species [4,5].
The possible accepted etiologies for the occurrence of feline lymphoma are viral immunosuppression, and the feline leukemia virus (FeLV) stands out as one of the most significant inducers of this disease [6,7]. This virus was cited in approximately 70% of cats with lymphoma. However, this reality is modifying since only 25% of cats with lymphoma are FeLV-positive [2,8]. Another virus possibly involved with the emergence of lymphomas is the feline immunodeficiency virus (FIV). It is known that approximately 20% of animals with lymphoma in the United States are seropositive for antibodies against FIV [2].
The average age of patients diagnosed with lymphoma is 8 to 10 years [3,9]. However, it varies with the form of the disease, and its etiology can strongly influence the onset of clinical signs [9]. According to [5], there is no evidence for racial or sex predisposition. These authors also claim that neutered males are slightly more affected by lymphoma, especially the alimentary type.
The lymphoma diagnosis is performed by clinical history, physical examination, laboratory and imaging tests, aspiration cytology, biopsy, and immunohistochemistry [8]. The treatment consists of chemotherapy protocols, usually with combined medicines, with no evidence that the associated surgical procedure is more effective than chemotherapy alone [9].
Nevertheless, antineoplastic medicines cause different toxic effects, especially regarding liver parenchyma [10] and animals with viral diseases, such as FIV and FeLV. The hepatotoxicity of chemotherapeutic medicines generally coincides with the increase in serum enzymes, such as alanine aminotransferase (ALT) and alkaline phosphatase (AP) [11]. Therefore, the elevation of the ALT and AP enzymes in the first chemotherapy sessions may indicate the toxic action of these medicines on the liver [11,12]. Myelotoxicity is another frequent and severe limiting factor of chemotherapy, impairing treatment efficacy and increasing the chances of metastases [13]. Additionally, it can lead the animal to death due to septic neutropenia [14]. Neutropenia is dose-limiting and can provoke septicemia with a risk of death for the patient [15].
Within this context, complementary therapies gain ground both as a primary or complementary treatment for cancer patients since they do not present side effects and they stimulate the immune system, improving life quality and, as a consequence, increasing the patient’s survival [16]. Viscum album is the plant most used in the world for the complementary treatment of cancer, with promising results recorded both as a curative or palliative strategy [17-19]. It is used in diverse injectable commercial forms, presenting a bidirectional effect to the treated patient. This medicine presents selective cytotoxicity, being aggressive only against the tumoral cells. It also presents immunomodulatory and anti-inflammatory activities [16].
[20] associated Viscum album with the traditional chemotherapy in dogs and observed a decrease in the total treatment time, reducing the chemotherapy side effects, such as leukopenia.
The objective of this study was to report the case of a domestic feline positive for FIV and FeLV, diagnosed with lymphoma, and successfully treated by injectable homeopathy.
Case Report
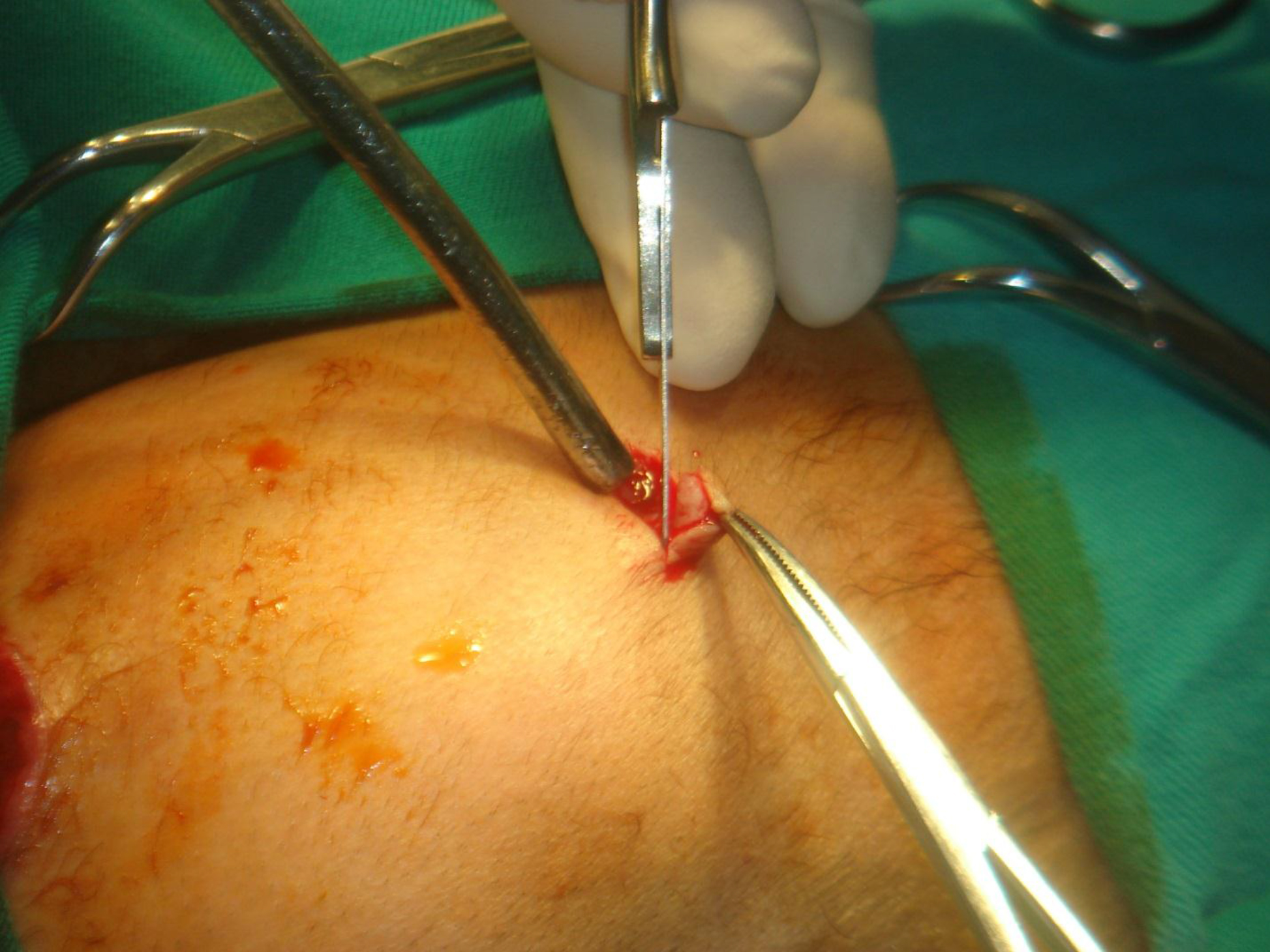
A 4-year-old male feline weighing 4.6 Kg, and positive for FIV and FeLV was seen at NaturalPet Clinic in Brasilia, Brazil. The animal has a history of difficulty swallowing concomitant with inappetence and respiratory difficulty. On physical examination, the animal was tachypneic with abdominal breathing, presented pale mucosa, CRT 3″, cardiac auscultation within the normal range considering age and species, mild dehydration, infarcted bilateral submandibular lymph nodes, and absence of pain on abdominal palpation. The examination of the oral cavity showed increased volume on the lower right side of the soft palate, small ulcerated portion, and hyperemic mucosa with apparent edema (Figure 1). Blood was collected for laboratory tests of complete blood count and biochemical measurements of alanine aminotransferase (ALT), alkaline phosphatase (AP), urea, and creatinine. The patient was also referred for a contrast-enhanced computed tomography. After the test results, the animal was referred for punch incisional biopsy (4 mm) and dental treatment, and the material was directed to histopathology. Subsequently, the treatment protocol was established through veterinary homeopathy. The following medicines were also prescribed, subcutaneously: Viscum album D3 (1×10-3), D6 (1×10-6), D9 (1×10-9), D12 (1×12-12), and D30 (1×10-30) (Injectcenterâ), a combination of two ampoules, once a day, for 60 days; Arnica montana D4 (1×10-4) (Injectcenterâ), one ampoule, once a day, for seven days; Apis melifera D4 (1×10-4) (Injectcenterâ), one ampoule, once a day, for seven days; Mercurius solubilis D18 (1×10-18) (Injectcenterâ), one ampoule, once a day, for 20 days. In addition, Stomorgylâ 10, ½ tablet every 24 hours, for seven dias; Omega 3 1000 mg, one capsule, once a day, for 60 days; and Vitamin C 500 mg, one tablet, once a day, for 30 days, were orally prescribed. After five months, the animal returned to the clinic complaining of discomfort in chewing. On the physical examination, the animal presented an ulcerated lesion on the contralateral side of the initial lesion (Figure 2). The same initial treatment was initiated for additional 12 weeks. The day after the evaluation, the animal was submitted to dental treatment to extract molar and premolar teeth and cauterize the injured region.
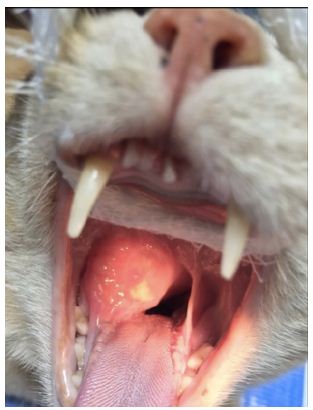
Figure 1: Presence of slightly ulcerated and contaminated nodule in the oral cavity of the cat.
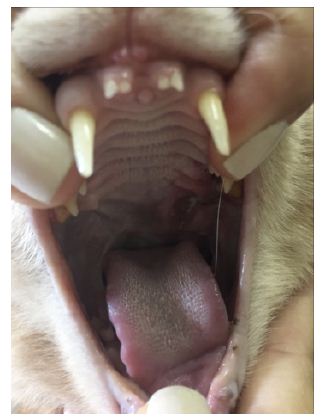
Figure 2: Presence of ulcerative lesions, represented by the white color arrow, in the initial portion of the soft palate and final portion of the hard palate (left side). On the right side of the image, represented by the green arrow, healed tissue previously affected by lymphoma.
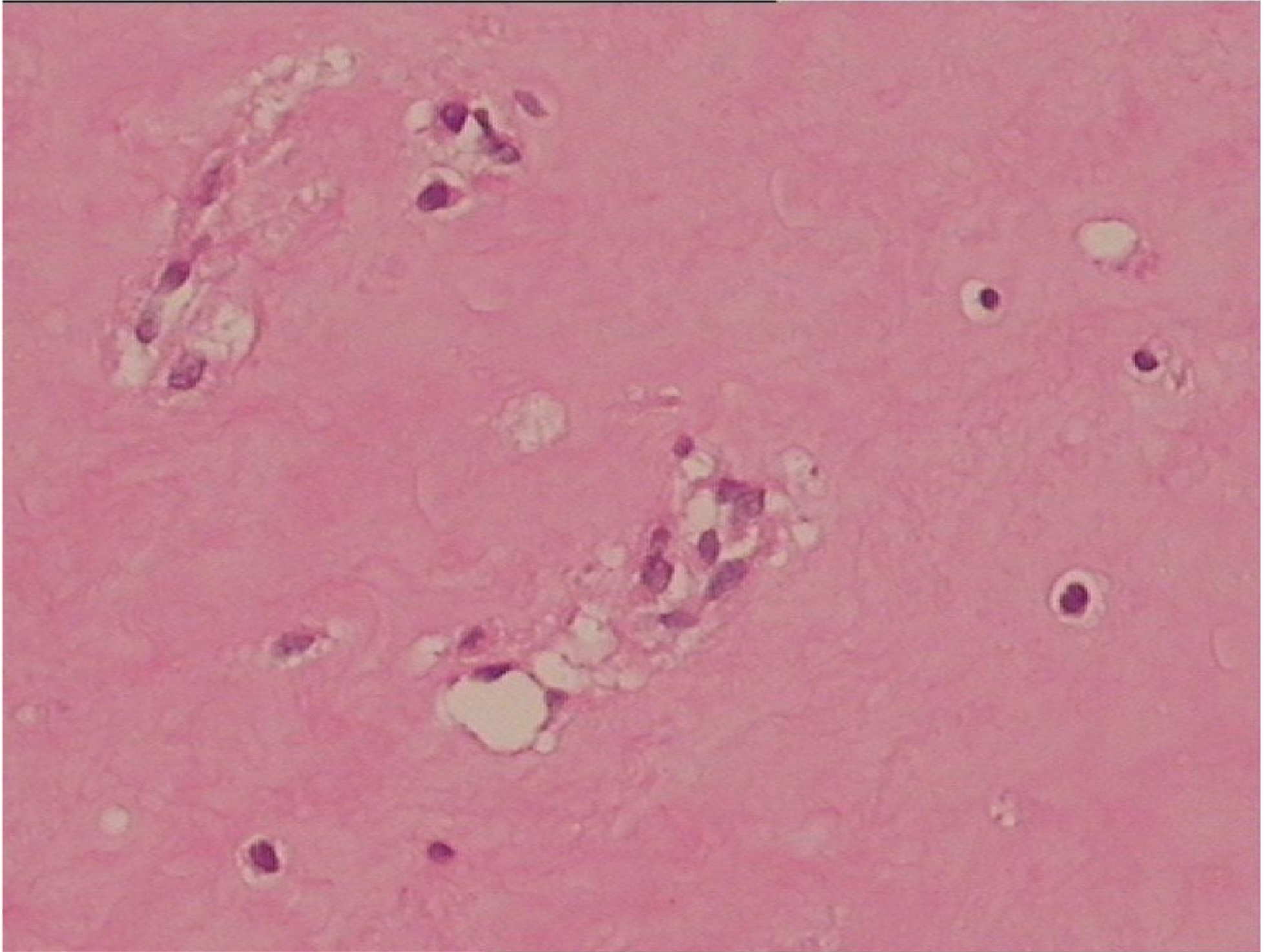
Results
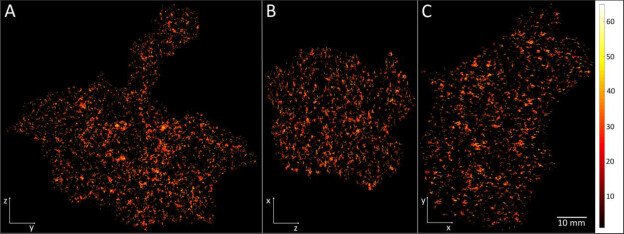
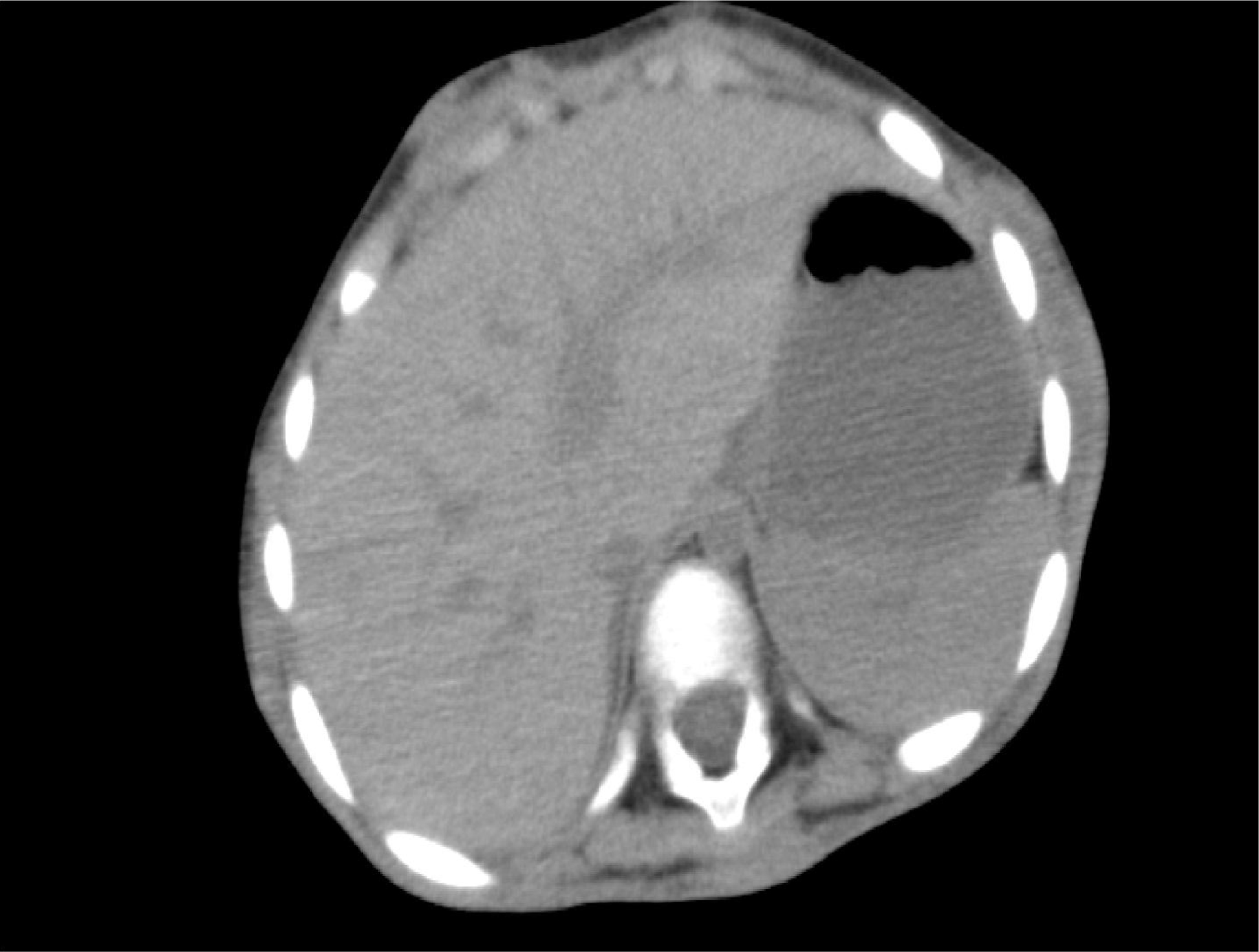
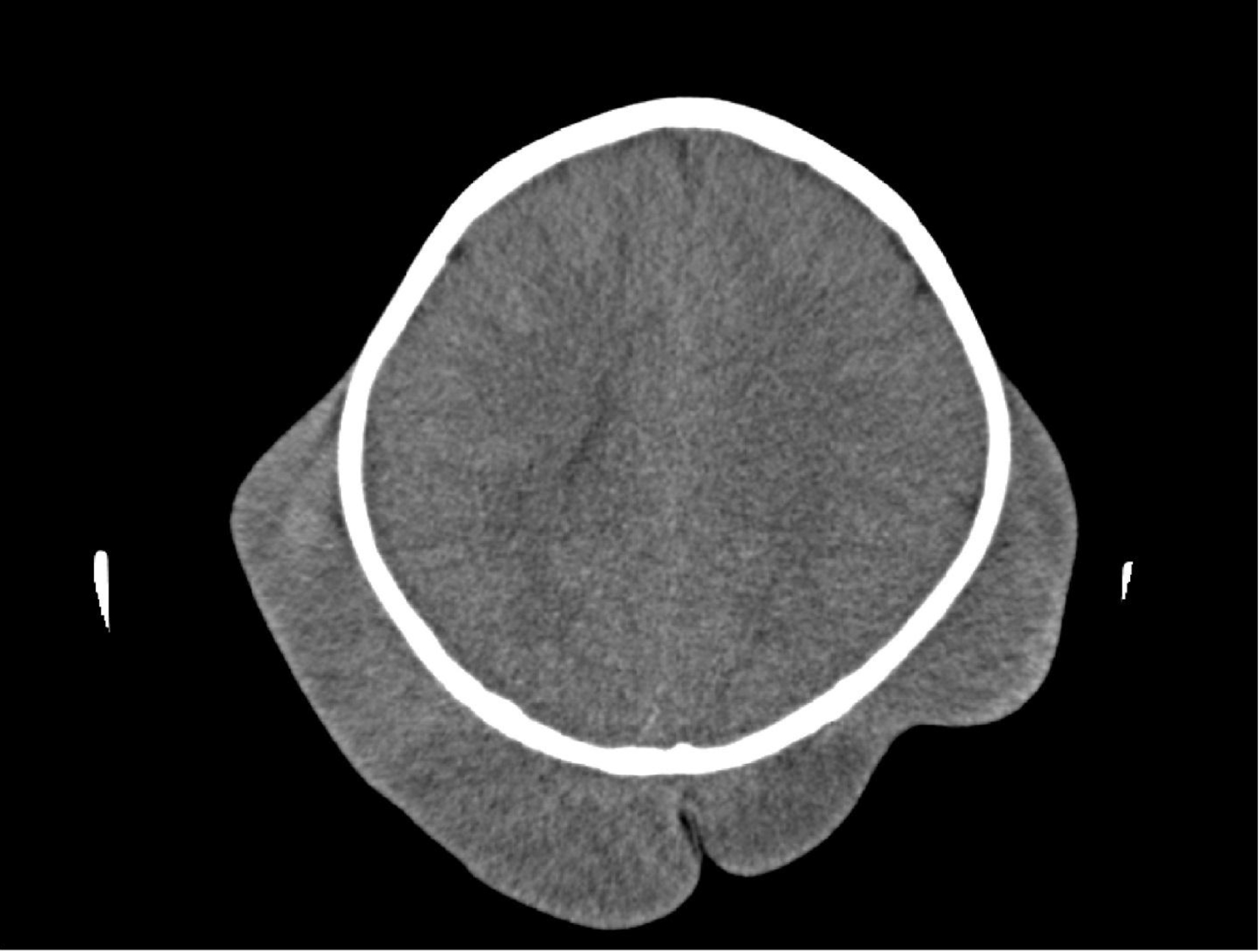
Contrast-enhanced computed tomography images (Figure 3) showed neoformation with an irregular shape, with venous contrast hyper-uptake presenting hypodensity areas in its interior, measuring approximately 3.0 cm in height x 3.5 cm wide x 4.8 cm in length, and located in the right submandibular lymph nodes topography. Signs of invasion of the neoformation mentioned above into the oropharyngeal region were observed, presenting signs of partial obstruction of the nasal choanae. The conclusion of the exam was suggestive of neoformation in the right submandibular lymph nodes topography, followed by the obstruction of the nasal choanae by a mass, as previously described. The results of the blood tests are shown in Table 1.
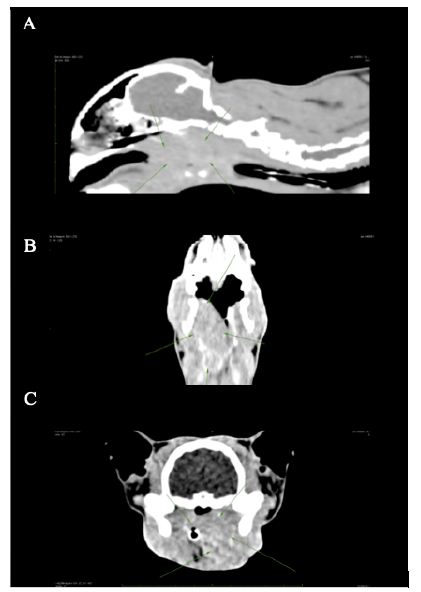
Figure 3: (A) Image in right longitudinal section (head and neck) – presence of a mass. (B) Ventral cross-sectional image of the animal’s head – presence of a mass on the left side. (C) Cross-sectional image of the sinus of the face – presence of a mass in the left sinus.
Table 1: Blood test data of a 4-year-old male feline, positive for FIV and FeLV, seen at NaturalPet Clinic in Brasilia, Brazil.
| |
May/2016
|
July/2016 |
September/2016 |
October/2016 |
January/2017 |
April/2017
|
| Red blood cells (mL) |
7,690,000
|
8,460,000 |
8,020,000 |
6,050,000 |
7,200,000 |
6,450,000
|
| Hemoglobin (g/dL) |
11
|
11.5 |
11.3 |
9.2 |
10.3 |
9.3
|
| Hematocrit (%) |
31.3
|
36.6 |
35 |
25.8 |
31.1 |
26.2
|
| MCV (g/dL) |
40.75
|
42.25 |
43.64 |
42.64 |
43.19 |
40.62
|
| MCHC (g/dL) |
35.14
|
31.51 |
32.29 |
35.66 |
33.12 |
35.5
|
| Leukocytes (mL) |
4,500
|
6,700 |
9,500 |
4,600 |
6,000 |
7,000
|
| Eosinophils (mL) |
585
|
402 |
0 |
506 |
720 |
630
|
| Lymphocytes (mL) |
1,800
|
2,278 |
855 |
1,794 |
1,440 |
1,750
|
| Platelets (mL) |
16,000
|
301,000 |
230,000 |
128,000 |
264,000 |
368,000
|
| TPP (dL) |
11.2
|
7.0 |
9.8 |
8.0 |
6.4 |
8.8
|
| ALT (U/L) |
55
|
** |
** |
** |
33 |
53
|
| Creatinine (mg/dL) |
1.5
|
** |
** |
** |
1.34 |
1.76
|
| AP (U/L) |
13
|
** |
** |
** |
17 |
24
|
| Urea (mg/dL) |
51
|
** |
** |
** |
53 |
31
|
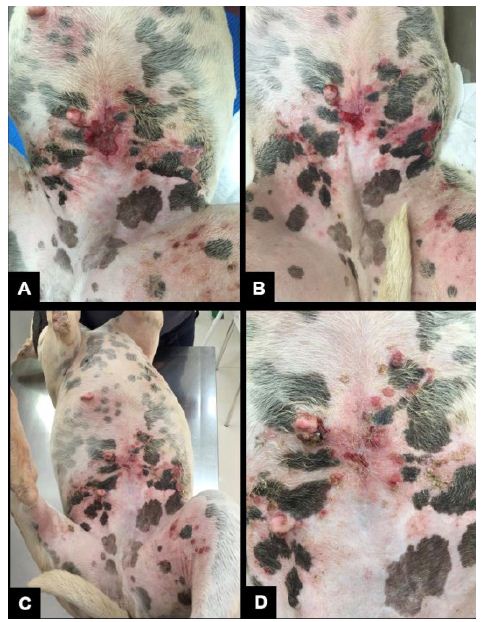
One week after the biopsy procedure and treatment initiation, the animal returned to the clinic, and the lesion was much smaller (Figure 4A). The clinical improvement can be seen in Figure 4, from the first week after the Viscum album therapy initiation until the 28th day of treatment, when the initial lesion was healed. The biopsy result was conclusive for lymphoma. The patient was followed up with complete blood count tests. The Viscum album applications should have happened daily, as per the veterinarian’s recommendation. However, the tutor of the animal discontinued the treatment, on her own, from the moment the lesion healed.

Figure 4: Lesion 1 (right side) – Evolution of the treatment and its response. (A) Lesion appearance seven days after treatment initiation. (B) Lesion appearance 14 days after.
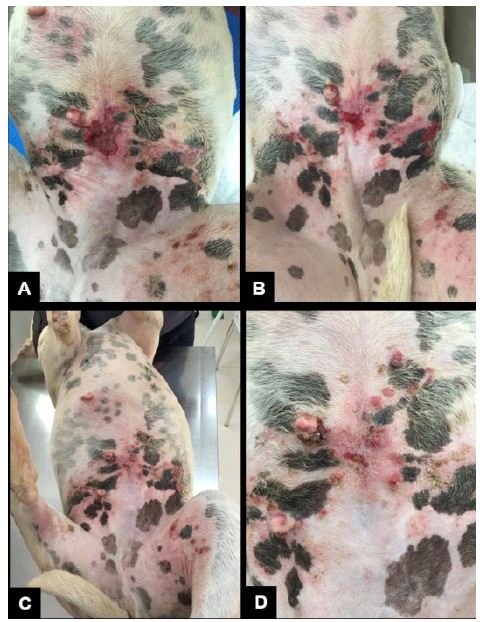
After restarting the treatment protocol and extracting the teeth, treatment evolution occurred in three weeks (Figure 5). The tutor continued the treatment for 60 days, and complete lesion healing was observed. Also, the patient remained well for another 36 months and presented normal appetite, water intake, urination, and defecation until he died with severe anemia associated with stage 3 kidney disease.
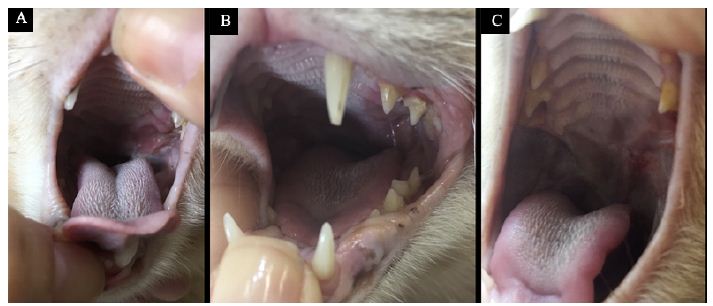
Figure 5: Lesion 1 (left side) – Evolution of the treatment and its response. (A) Lesion appearance seven days after treatment initiation. (B) Lesion appearance 15 days after treatment initiation. (C) Lesion appearance 28 days after treatment initiation.
Discussion
Lymphoma is the hematopoietic neoplasm most commonly diagnosed in domestic cats, comprising approximately one-third of all tumors in this species. FeLV-positive animals continue to be potential candidates for lymphoma and feline leukemia involvement [21]. Lymphoma is a systemic neoplasm, and the basis of treatment is chemotherapy. Its proper use promotes increased longevity and quality of life of cancer patients, and in some cases, even achieves the complete cure of cancer [22]. The chemotherapeutic treatment aims to induce complete and lasting remission of the neoplasm, and in cases of recurrence, reinduce its remission [23].
Numerous treatment protocols have been reported for feline lymphoma with varied results. The reported literature includes a wide variety of chemotherapy protocols associated or not with corticosteroids that are typically extended for a year or more [21]. Many of these protocols have different side effects, which are limiting factors for FIV and FeLV patients due mainly to the immunosuppression caused by chemotherapy and corticosteroids. In contrast to these authors, the present report describes a case of lymphoma in an FIV and FeLV positive cat treated by the Viscum album therapy with satisfactory results. Furthermore, it is important to emphasize that the therapy used did not have side effects for the patient, nor does it have contraindications.
Also, according to [24-26], overall responses reported for feline lymphoma treated with various chemotherapy protocols vary widely, with median survival times ranging from 50 to 388 days. On the other hand, the present study reports that besides being FIV and FeLV positive, the animal was treated by complementary medicine, basically by the Viscum album therapy. Under this protocol, the patient presented a survival three times greater than the maximum survival recorded for patients treated exclusively by the conventional treatment in FIV and/or FeLV positive or negative animals.
Additionally, our findings are corroborated by [18], who also recorded disease resolution, increased life expectancy, and no side effects when using injectable Viscum album and Magnesia phosphorica for treating feline alimentary lymphoma. Therefore, these are promising data that point to the importance of ongoing studies on the effects of the Viscum album therapy on cancer patients to allow for meaningful decision-making and efficient disease treatment.
Conclusion
This study raises another possibility for treating patients to whom conventional therapies do not contemplate the quality of life associated with survival. Homeopathy is an excellent therapeutic tool for patients with pre-existing diseases, debilitated, or even as a complementary therapy for conventional treatments. Therefore, we propose further studies in the area so that the results obtained in this work are better validated.
References
- Vail DM, Ogilvie GK (1998) Lymphoid neoplasias. In: Manual saunders: small animal clinic, Eds., Bichard, S. J. and Sherding, R.G. Roca: São Paulo, Brazil. 218-225.
- Court EA, Watson ADJ, Peaston AE (1997) Retrospective study of 60 cases of feline lymphosarcoma. Aust Vet J 75: 424-427. [crossref]
- Gabor LJ, Malik R, Canfield PJ (1998) Clinical and anatomical features of lymphossarcoma in 118 cats. Aust Vet J 76: 725-732. [crossref]
- Vonderhaar MA, Morrison WB, Lymphosarcoma (2002) In Cancer in dogs and cats: medical and surgical management, Ed., Morrison, W.B. Jackson Hole, WY: Teton New Media. 641-670.
- Norsworthy GD, Grace SF, Crystal MA, Tilley LP (2011) The feline patient. ed. Wiley – Blackwell: Iowa.
- Lutz H, Addie D, Belák S, Boucraut-Baralon C, Egberink H, et al. (2009) Feline leukaemia. ABCD guidelines on prevention and management. J Feline Med Surg. 11: 565-574. [crossref]
- Hartmann K (2012) Feline leukemie virus infection. In Infections diseases of the dog and cat, Ed., Greene, C.E. Missouri, USA: Elsevier.
- Bado AS (2011) Alimentary lymphoma in cats. Undergraduate thesis (Undergraduation in Veterinary Medicine) – Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil. 38p.
- Wilson HM (2008) Feline Alimentary Lymphoma: Demystifying the Enigma. Top Companion Anim Med. 23: 177-184. [crossref]
- Barger AM, Grindem CB (2000) Hematologic abnormalities associated with cancer therapy. In Schalm’s Veterinary Hematology, Eds., Feldman, B.F., Zinkl, J.G., and Jain, N.C. 5 ed. Canada: Lippincott Williams.
- Rodaski S and Werner J (2008) Skin neoplasia. In Oncology in dogs and cats, Eds., Daleck, C.R., De Nardi, A.B. and Rodaski, S. Sao Paulo, Brazil: Roca. 253-279.
- Araujo GG (2009) Feline lymphoma. Undergraduate thesis (Undergraduation in Veterinary Medicine) – Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil. 45 p.
- Hernandez JDT (1994) Uso clínico de los factores de crescimento hematopoyético. Iatreia 7: 173-180.
- Lanore D, Delprat C (2004) Anticancer chemotherapy. Roca: São Paulo, Brazil.
- Nelson RW, Couto CG (2003) Chemotherapy complications of cancer. Small animal internal medicine. 3 ed. Mosby: St. Louis.
- Valle ACV, Andrade RV, Lopes D, Sibata M, Carvalho AC (2018) Ultradiluted Viscum album in the treatment of myeloma in a dog – case report. In the Proceedings of the Supportive care makes excellent cancer care possible – MASCC. Viena, Austria.
- Valle ACV, Lima L, Bonamin L, Brunel H, Barros A, et al. 2020. Use of Viscum album in the Integrative Treatment of Cholangiocarcinoma in a Dog (Canis familiaris) – Case Report. Adv Complement Alt Med 5: 476-481.
- Carvalho A, Valle ACV (2021) Treatment of Alimentary Lymphoma in Cat (Felis catus) by Injectable Homeopathy – Case Report. Integr J Vet Biosc 5: 1-6.
- Valle ACV, Carvalho AC (2021) Ultra-diluted Viscum album in the treatment of cutaneous melanoma in a dog (Canis familiaris) – Case report. Paripex Indian J Res 10: 1-4.
- Lefebvre GNF, Bonamin LB, Oliveira CM (2007) Treatment of transmissible venereal tumor (TVT) using Viscum album in combination with chemotherapy. Rev Clin Vet 70: 78-86.
- Collette SA, Allstadt SD, Chon EM, Vernau W, Smith AN, et al. (2016) Treatment of feline intermediate‐ to high‐grade lymphoma with a modified University of Wisconsin–Madison protocol: 119 cases (2004–2012). Vet Comp Oncol 14: 136-146.
- Couto CG (2000) Advances in the treatment of the cat with lymphoma in practice. J Feline Med Sur 2: 95-100. [crossref]
- Withrow SJ, Vail DM (2007) Withrow & MacEwen’s Small Animal Clinical Oncology. 4. ed. St. Louis, MO: Saunders Elsevier.
- Simon D, Eberle N, Laacke-Singer L, Nolte I (2008) Combination chemotherapy in feline lymphoma: treatment outcome, tolerability, and duration in 23 cats. J V Intern Med 22: 394-400. [crossref]
- Krick EL, Moore RH, Cohen RB, Sorenmo KU (2011) Prognostic significance of weight changes during treatment of feline lymphoma. J Feline Med Surg 13: 976-983. [crossref]
- Krick EL, Cohen RB, Gregor TP, Salah PC, Sorenmo KU (2013) Prospective Clinical Trial to Compare Vincristine and Vinblastine in a COP‐Based Protocol for Lymphoma in Cats. J Vet Intern Med 27: 134-140. [crossref]